A therapist's job is an odd one. In fact, my job is officially to work myself out of a job. Weird, huh? But true. My job is to support people in "getting better," however that is defined, and then watch them walk away. When I started this blog, it was called Within Four Walls, because part of what I wanted to be able to communicate was the power, and for me, joy, of working with people with eating disorders. A couple years ago, I was at a local gathering of people who treated or wanted to treat eating disorders, and I was appalled when I heard a therapist state, "Oh, nobody with an eating disorder ever gets better anyway." I had to bite back my desire to tell her to never, ever see another eating disorder patient. But, that is an a common misconception; that eating disorders are generally untreatable. So not true.
Recently, I had a final session with a woman who I have been working with for years. Obviously, I don't want to disclose details about this woman, but also want to say enough for you, the reader, to understand why the statement that people with eating disorders don't get better is so wrong. When I met this woman, she was a shell of a person, in every way.
Today, she left to move to another place to start a graduate program. And, when you hang out with someone every week, or so, for a few years, you lose track of all the changes that happen. It's not until you look back at where things started that it really strikes you, the therapist, just how much changed. I'm sure if anyone were going to, this woman fit the profile of the person who would "never get better." The severity of the illness and it's impact on her physiology, the overall impairment in functioning in her life; there was a lot going against her. When I look back, I see that it didn't look good all those years ago. But, years passed, and in reality, she has been recovered from her eating disorder for years. It has not been the focus on her therapy work for a long time and many situations have shown she truly is in recovery. Therapy became about life and rebuilding, and she did.
In the final session, she tried to give me the primary responsibility for "getting her better." Nope, that wasn't going to happen! It wasn't me. So, what was it? Well, first it was that she wanted to get better. She started the process, she continued the process, she hung in there through hairy moments and good. She drove the process. If you really think about it, what is eating disorder treatment? Sure, to a certain extent we help people "re-learn how to eat." But, really, everyone KNOWS how to eat. We don't have super Jedi mind tricks that somehow make someone eat again.
So, what is it that we do? If you look at psychology, and therapy in general, I'd hate to even try to count the number of approaches that us therapists can be trained in. There's about every cute little combination of letters in the book, all labeling some therapeutic approach that is destined to be the NEXT, BEST THING!
But a couple years ago, when I was panicking about a patient and whether I was doing things "right," and was told by some clinicians that I was doing things wrong, another clinician pointed out the research that basically says that we as therapists can do almost anything, within reason, and as long as we believe it works, and then our patients believe it works; well, it tends to work.
So, you take all those therapy approaches....CBT, IPT, DBT, ACT, ABCDEFG (that's not really one), and they all work, really. But what I believe works, what I believe therapy offers people, is a relationship. That's what therapy is, and that's what we, as people, need (except, as I always tell my clients, there is this guy that lives in a cave outside of Nederland, CO...or at least he did when I was in grad school...and there are a few people like him that seem to not need relationships....but those folks are rare). So, that's what I offered to this woman. I did not "make her better." I gave her a relationship, and she chose to use that relationship to change her life. And, in my experience, the change that comes from the power of the relationship is long-standing. So, I don't worry that she will return to her eating disorder. I truly believe she is recovered. And that puts a huge smile on my face, knowing where things started. She chose her life over her eating disorder.
So, I was reminded by this patient the true power of what happens Within these, and all other, Four Walls.
Wednesday, July 31, 2013
Wednesday, July 17, 2013
What should my child weigh?
As I was thinking more about the last post, I realized I wanted to share some more information related to kids and their weights. I'll begin with a story:
A few weeks ago, I was talking to a physician about a referral. He let me know that this teenager had lost a significant amount of weight....I'll make up numbers here....let's say she was 5'2 and 120# prior to her weight loss. She lost to 100#, was admitted to the hospital, partially refed, and now will be seen for outpatient follow up. The doctor's stance as not uncommon, and amounted to this: We'll say she gained to 110# in the hospital and this is her new "goal weight," because, in his words, 110# is a reasonable weight for a teenager that is 5'2.
And for me, there's the internal sigh, knowing there's little I can do to override this physician's understanding of appropriate weight, or eating disorder terms, "goal weight." Reality is that very few health professionals, of any discipline, have the opportunity to learn about eating disorder treatment while in training. The main way of learning about ED treatment is through specialty rotations or job placements. So, sadly, the norm is that health professionals are more strongly influenced by the media, and thus the diet industry, than by solid science.
So, everyone knows about those lovely height/weight tables, right? Pick an age, pick a height, and voila! A piece of paper will tell you what you should ideally weight. Okay, well, the name for that table is the MetLife Height/Weight table, and yep, MetLife is an insurance company. So, these were tables designed by an insurance company to protect their interests, and are based in the (flawed) theory that lower weight has lower health consequences. Which is actually completely incorrect, but that's a whole 'nother post.
The theory here is that we can take ALL THE HUMANS IN THE WORLD, and a piece of paper should tell us what we SHOULD weigh. (I hope the sarcasm here is palpable!). This is illogical. So, if you follow that handy dandy piece of paper, yes, the doctor's statement above is "correct." Because that table will say about 5'2, 110# for a female. The problem here is that this particular teenager was at 120# prior to her disorder, so what is to say she SHOULD now weigh less as a result of having a disorder.
What's the real answer?
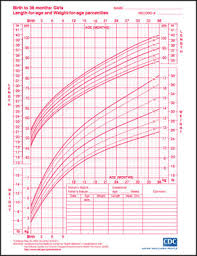 It's really pretty straightforward, though it does involve another handy dandy piece of paper. The new piece of paper is a CDC Growth Chart for boys or girls. Each time your child sees his/her pediatrician, height and weight is recorded on one of these charts. In my experience, most kids will actually track pretty well along a particular percentile in height and in weight.
It's really pretty straightforward, though it does involve another handy dandy piece of paper. The new piece of paper is a CDC Growth Chart for boys or girls. Each time your child sees his/her pediatrician, height and weight is recorded on one of these charts. In my experience, most kids will actually track pretty well along a particular percentile in height and in weight.
So, let's make our female teenager above 14 years old. At 120#, she would be in the 25%ile for height and I'll say 62%ile for weight (this is a rough estimate just eyeballing the chart). So, let's say she lost weight and then was hospitalized and now at age 15, she is entering outpatient treatment at 110#. Reality is that her height likely remained the same, because maintaining too low a weight stunts height, which, again, is a whole 'nother post. But, at 15, 110# puts her at the 33rd-ish percentile.
Assuming this teenager had tracked at the 55th-65th percentile throughout her childhood, to now say she is healthy in the 33rd percentile, simply because a height/weight chart says that is good, is irrational. Teenagers are supposed to continue to gain, both in height and weight. But, unfortunately, health professionals, and then parents, often think the child/teenager is "fine" as long as he/she meets the cultural expectations for weight.
To get my point across solidly, let's say that there's a handy dandy MetLife chart for shoe size, or even height for age. So, let's say that at age 16, the chart says I should be 5'4 (average height for women), and a shoe size of 7.5. Well, good news! My shoe size actually is 7.5, so woo hoo! I did it! But, sadly, I suffer from height failure, and am only 5'2 (or 5'3, if the doctor is being kind). But the chart says I need to be 5'4....so, I guess I better get stretching. I better have someone pull on my hands and someone else pull on my legs until I get there, right? Ouch.
That sounds nutty when it comes to height. But my point is that it is equally nutty when it comes to weight. If a child/teen has always tracked at the 95%ile for height or weight, then they are HEALTHY at 95%ile, even if our society begs to differ. And, if they have always tracked at the 5th%ile, then they are HEALTHY there, which our society fully supports, at least with respect to weight.
Now, parents, please do not now go demand your child's height/weight records from their pediatrician. You don't need to drive yourself nuts analyzing it. Just know that that reference point is available, and is much more accurate than a chart created by an insurance company. Parents, keep your focus on helping your child eat when he/she is hungry and stop when he/she is full. If your child does this, he/she will maintain his/her natural weight, well, naturally.
But, health professionals, if you are relying on the MetLife tables, or the other handy dandy estimates that are out there, please reconsider. Humans should be judged against their own history (growth charts), not an average of people put into table form (MetLife Height/Weight chart).
A few weeks ago, I was talking to a physician about a referral. He let me know that this teenager had lost a significant amount of weight....I'll make up numbers here....let's say she was 5'2 and 120# prior to her weight loss. She lost to 100#, was admitted to the hospital, partially refed, and now will be seen for outpatient follow up. The doctor's stance as not uncommon, and amounted to this: We'll say she gained to 110# in the hospital and this is her new "goal weight," because, in his words, 110# is a reasonable weight for a teenager that is 5'2.
And for me, there's the internal sigh, knowing there's little I can do to override this physician's understanding of appropriate weight, or eating disorder terms, "goal weight." Reality is that very few health professionals, of any discipline, have the opportunity to learn about eating disorder treatment while in training. The main way of learning about ED treatment is through specialty rotations or job placements. So, sadly, the norm is that health professionals are more strongly influenced by the media, and thus the diet industry, than by solid science.
So, everyone knows about those lovely height/weight tables, right? Pick an age, pick a height, and voila! A piece of paper will tell you what you should ideally weight. Okay, well, the name for that table is the MetLife Height/Weight table, and yep, MetLife is an insurance company. So, these were tables designed by an insurance company to protect their interests, and are based in the (flawed) theory that lower weight has lower health consequences. Which is actually completely incorrect, but that's a whole 'nother post.
The theory here is that we can take ALL THE HUMANS IN THE WORLD, and a piece of paper should tell us what we SHOULD weigh. (I hope the sarcasm here is palpable!). This is illogical. So, if you follow that handy dandy piece of paper, yes, the doctor's statement above is "correct." Because that table will say about 5'2, 110# for a female. The problem here is that this particular teenager was at 120# prior to her disorder, so what is to say she SHOULD now weigh less as a result of having a disorder.
What's the real answer?
So, let's make our female teenager above 14 years old. At 120#, she would be in the 25%ile for height and I'll say 62%ile for weight (this is a rough estimate just eyeballing the chart). So, let's say she lost weight and then was hospitalized and now at age 15, she is entering outpatient treatment at 110#. Reality is that her height likely remained the same, because maintaining too low a weight stunts height, which, again, is a whole 'nother post. But, at 15, 110# puts her at the 33rd-ish percentile.
Assuming this teenager had tracked at the 55th-65th percentile throughout her childhood, to now say she is healthy in the 33rd percentile, simply because a height/weight chart says that is good, is irrational. Teenagers are supposed to continue to gain, both in height and weight. But, unfortunately, health professionals, and then parents, often think the child/teenager is "fine" as long as he/she meets the cultural expectations for weight.
To get my point across solidly, let's say that there's a handy dandy MetLife chart for shoe size, or even height for age. So, let's say that at age 16, the chart says I should be 5'4 (average height for women), and a shoe size of 7.5. Well, good news! My shoe size actually is 7.5, so woo hoo! I did it! But, sadly, I suffer from height failure, and am only 5'2 (or 5'3, if the doctor is being kind). But the chart says I need to be 5'4....so, I guess I better get stretching. I better have someone pull on my hands and someone else pull on my legs until I get there, right? Ouch.
That sounds nutty when it comes to height. But my point is that it is equally nutty when it comes to weight. If a child/teen has always tracked at the 95%ile for height or weight, then they are HEALTHY at 95%ile, even if our society begs to differ. And, if they have always tracked at the 5th%ile, then they are HEALTHY there, which our society fully supports, at least with respect to weight.
Now, parents, please do not now go demand your child's height/weight records from their pediatrician. You don't need to drive yourself nuts analyzing it. Just know that that reference point is available, and is much more accurate than a chart created by an insurance company. Parents, keep your focus on helping your child eat when he/she is hungry and stop when he/she is full. If your child does this, he/she will maintain his/her natural weight, well, naturally.
But, health professionals, if you are relying on the MetLife tables, or the other handy dandy estimates that are out there, please reconsider. Humans should be judged against their own history (growth charts), not an average of people put into table form (MetLife Height/Weight chart).
"The Childhood Obesity Epidemic" and Eating Intuitively
Our society has done a wonderful job scaring everyone about rates of childhood obesity. I haven't delved into the research myself and really looked at the extent to which children are at higher weights/BMIs, etc., but I feel confident that the way our society is responding to any issues that might be present is not that beneficial. Parents are learning they need to restrict their child's food intake and access to food. They are advised by doctors, therapists, and the media, to limit what their child has access to and control food intake.
But let's think about this. Go back to being a child or teenager. Think of what happened when your parents told you you couldn't do something, and particularly when they told you you couldn't do something that all your friends were doing. Right, you rebelled against that, or at least thought about it.
So, when, as a parent, you try to limit your child's access to soda, fast food, pizza, "junk food," etc., the greater risk is that you will accomplish pushing your child towards those foods as they fight back against the restriction. The diet industry, and thus most health professionals, will identify all these foods as "bad." We are instructed to not eat them, and it is implied that it is "bad" if we do. The shame is compounded when it is then implied that to allow access to these foods is "bad" and that having a child eat these foods, especially when they more than society says is idea is "bad." That's a lot of "bad"s, for both parent and child.
It is true that not all foods offer the same nutritional value. Yes, there are limits, and sometimes significant limits, to the nutritional value of the foods that have been identified as bad. However, these foods are present in our world, and the black and white view of "don't eat them" isn't very likely to work out well. So what is a parent to do instead?
Rather than focusing heavily on the foods that your child is eating, focus instead on their hunger and fullness level. Kids are born intuitive eaters. Your babies and young children ate intuitively. They asked for food when they were hungry, and they stopped eating when they were full. They didn't have the neuroses we adults have about foods because, to kids, food is just food. However, as they grow up in our culture and hear about good and bad foods, and external forces begin to impact when they start and stop eating, they lose their ability to follow their hunger and fullness cues. Telling your child she has to eat everything on her plate overrides her fullness cues. Telling your child he cannot eat, or cannot eat ____ when he's hungry overrides his hunger cues. But you can help your kids go back to those cues by talking to them not about the food, but instead about how hungry and full they are.
How does this look? You are concerned your child is overeating, so you ask him whether he's still hungry. If he says yes, you cannot know for sure whether that is the truth, but you can know that you are helping him to think about that factor. Over time, he is more likely to think about this variable when he is making food choices. It will help if this is how you approach food yourself so it is modeled for your child.
It's not as much about what he/she is eating, but the physical cues that are driving the eating behavior. If you focus on what and how much he/she eats, your child is more likely to feel criticized and blamed, particularly if he/she actually is eating due to hunger! Certainly, have foods with high nutritional value available to your kids, and serve these foods. But, I think we all know that there are times when fast food is what is most available, and really, in the end, fast food is a source of protein, carbs, fat, and more so recently, fruits and vegetables. So, it doesn't have to be a big deal. It's not ideal to eat them all the time, but reality is that it also is not a good idea to eat broccoli all the time (I don't know why; I always pick on broccoli! I just have a vendetta against that little green tree....) Eating any one source of food repeatedly limits nutrition, so eat fast food, and broccoli, as part of a varied diet, and you will be fine.
I hope, moving forward, parents will question more trying to limit their child's food intake. I have seen this result in a variety of eating problems, and what is sad is that it is all well-intended and parents are directed to take these steps by health professionals. Again, remember that your babies and young children were intuitive eaters. Help them return to that if our society has overridden this natural way of being.
But let's think about this. Go back to being a child or teenager. Think of what happened when your parents told you you couldn't do something, and particularly when they told you you couldn't do something that all your friends were doing. Right, you rebelled against that, or at least thought about it.
So, when, as a parent, you try to limit your child's access to soda, fast food, pizza, "junk food," etc., the greater risk is that you will accomplish pushing your child towards those foods as they fight back against the restriction. The diet industry, and thus most health professionals, will identify all these foods as "bad." We are instructed to not eat them, and it is implied that it is "bad" if we do. The shame is compounded when it is then implied that to allow access to these foods is "bad" and that having a child eat these foods, especially when they more than society says is idea is "bad." That's a lot of "bad"s, for both parent and child.
It is true that not all foods offer the same nutritional value. Yes, there are limits, and sometimes significant limits, to the nutritional value of the foods that have been identified as bad. However, these foods are present in our world, and the black and white view of "don't eat them" isn't very likely to work out well. So what is a parent to do instead?
Rather than focusing heavily on the foods that your child is eating, focus instead on their hunger and fullness level. Kids are born intuitive eaters. Your babies and young children ate intuitively. They asked for food when they were hungry, and they stopped eating when they were full. They didn't have the neuroses we adults have about foods because, to kids, food is just food. However, as they grow up in our culture and hear about good and bad foods, and external forces begin to impact when they start and stop eating, they lose their ability to follow their hunger and fullness cues. Telling your child she has to eat everything on her plate overrides her fullness cues. Telling your child he cannot eat, or cannot eat ____ when he's hungry overrides his hunger cues. But you can help your kids go back to those cues by talking to them not about the food, but instead about how hungry and full they are.
How does this look? You are concerned your child is overeating, so you ask him whether he's still hungry. If he says yes, you cannot know for sure whether that is the truth, but you can know that you are helping him to think about that factor. Over time, he is more likely to think about this variable when he is making food choices. It will help if this is how you approach food yourself so it is modeled for your child.
It's not as much about what he/she is eating, but the physical cues that are driving the eating behavior. If you focus on what and how much he/she eats, your child is more likely to feel criticized and blamed, particularly if he/she actually is eating due to hunger! Certainly, have foods with high nutritional value available to your kids, and serve these foods. But, I think we all know that there are times when fast food is what is most available, and really, in the end, fast food is a source of protein, carbs, fat, and more so recently, fruits and vegetables. So, it doesn't have to be a big deal. It's not ideal to eat them all the time, but reality is that it also is not a good idea to eat broccoli all the time (I don't know why; I always pick on broccoli! I just have a vendetta against that little green tree....) Eating any one source of food repeatedly limits nutrition, so eat fast food, and broccoli, as part of a varied diet, and you will be fine.
I hope, moving forward, parents will question more trying to limit their child's food intake. I have seen this result in a variety of eating problems, and what is sad is that it is all well-intended and parents are directed to take these steps by health professionals. Again, remember that your babies and young children were intuitive eaters. Help them return to that if our society has overridden this natural way of being.
Subscribe to:
Posts (Atom)