Of course, Thanksgiving is a holiday dreaded by those with eating disorders. They are scared of the amount of food, what might happen with food, what family members will say to them about their eating. So, here's a few ideas for making Thanksgiving more enjoyable. (Please keep in mind, though, that if you are a patient in treatment, none of what I say should override any plans you have made with your treatment team.)
1. Yes, our society has made Thanksgiving about food. But, you can choose to make it about family, or time off work, or whatever you want to make it about. The food is just food.
2. Our society advocates for starving all day and then overeating the Thanksgiving meal. What I recommend to all my patients is that they treat Thanksgiving as just any other day and any other meal. So, eat meals and snacks throughout the day, and then view the Thanksgiving meal as just a normal meal.
3. That said, it is okay to overeat Thanksgiving some. What you want to protect yourself from is either restricting or bingeing. But, at the Thanksgiving meal, a lot of good foods you maybe don't normally have are available, so it's okay to eat more than usual. Nothing terrible will happen to your body, and in fact, your metabolism will just speed up in response.
4. Use family to support you when you are struggling. Before even getting to the Thanksgiving festivities, identify who is going to be your support person and let them know you have chosen them. When you are having a hard time, pull them off to the side and talk to them and let them help in whatever way.
a. If you are the family member who has been identified to help, remember this key phrase: "What
can I do to help?" This saves you from feeling like you need to fix everything, which would likely
frustrate your loved one with an eating disorder.
5. If it helps, plan out what you are going to eat before the meal itself so you are less likely to panic in the moment.
6. If you are doing Intuitive Eating, remember all foods are good foods, no foods are bad foods! You are "allowed" to eat anything no matter who or what has said something about that food. Eat when you are hungry, stop when you are full, and remember you can always have leftovers later.
7. If you are concerned about bingeing, and have the "last supper" mentality, wherein you feel pressured to eat more because you are afraid there you must eat it all while it is available, consider going ahead and making yourself a plate of leftovers before you eat your meal so you can be confident you can have later the foods you really enjoy. Yes, this will be unusual, but your family should be able to support you in taking this step as managing your eating disorder well.
But, most important, remember Thanksgiving is not truly about the food. You are there to spend time with family and/or friends and enjoy the day, or the day off, or whatever is enjoyable! Happy Thanksgiving!
Wednesday, November 21, 2012
Monday, November 19, 2012
News coverage, part II
The aforementioned news outlet has again contacted me to come on air, this time to address EDs in men. I spoke with the reporter at length, expressing my concerns about the previous story, and was told this reporter would not do the same thing. So, I agreed.
But, I just read the story in GQ that this reporter is basing her story on, and it is yet another ED story that talks about behaviors and weight, etc. (Why is it so rare that a news outlet can manage to pull off a story that does not glorify EDs??) And, as much as this reporter might agree to not do the same story, reality is I don't have any ability to reject participation once the interview is done.
So, the question is this: Does the benefit of talking about EDs in men outweigh the risks of the impact of another potentially glorifying story?
Please, thoughts?
But, I just read the story in GQ that this reporter is basing her story on, and it is yet another ED story that talks about behaviors and weight, etc. (Why is it so rare that a news outlet can manage to pull off a story that does not glorify EDs??) And, as much as this reporter might agree to not do the same story, reality is I don't have any ability to reject participation once the interview is done.
So, the question is this: Does the benefit of talking about EDs in men outweigh the risks of the impact of another potentially glorifying story?
Please, thoughts?
Wednesday, November 14, 2012
The person is not his/her disorder
Some of you may have seen the local news story about anorexia the other day. Of course, I support anyone with an eating disorder getting the support they need, but I found the news story to be so inappropriate in so many ways, a few of which I will detail here.
As my patients know, one of my huge pet peeves is the use of the words "anorexic" and "bulimic." When I wrote my dissertation, which was largely on cutting, I drove my advisor nuts because I refused to write the word, "cutter," and instead made my dissertation significantly longer, I am sure, by writing "individuals who engage in self-harm" and similar phrases. So, here's the point: Do you call someone who has cancer, cancer-ic? No, you don't. So, why would someone with anorexia be "an anorexic." The person is not his or her disorder, and in fact, identifying with the disorder is one of the major hurdles to overcome in treatment. So, hearing "anorexic" over and over was very upsetting. This patient did not need to identified as her disorder. She is a person, with a disorder; she is not actually a disorder.
News stories seem to feel such pull to glamorize eating disorders also. Maybe glamorize is not quite the right word. But, they feel the need to show exactly what symptoms the person engages in, his/her weight, etc. All the things that those with eating disorders compete over. So, maybe the news story helped those who know absolutely nothing about EDs understand what behaviors make up an ED, but I was frustrated because I knew those with EDs who were watching the story were being triggered right and left. Some simple research on the part of the reporters would have helped them understand the disorder better, and know what they decided to focus on not only is not unique, but likely triggering to others with the disorder about which they were trying to educate.
So, what could the story have been about instead? How about using this woman's story, without all the details, to present the message that there needs to be greater insurance coverage for treatment? There would have been a lot of benefit to trying to engage people in the fight against insurance companies, or to strengthen laws regarding mental healthy parity. People left that news story knowing what symptoms make up anorexia, and one individual that has the disorder. So much more good could have been done by focusing less on the details, and more on what needs to change within our healthcare system when it comes to eating disorder treatment and coverage.
I want to make it clear I am not criticizing the woman in the piece. She has an eating disorder and deserves access to treatment and, I'm assuming, took the steps she thought could help her get help. I'm criticizing those who were more in the position to treat this story differently, and create greater benefit.
Update: I was just called by the new outlet to come on air live for their follow up story. I refused on principle, and let them know my concerns with their approach to this story. So, hopefully the information I gave them will help change their approach in follow up.
As my patients know, one of my huge pet peeves is the use of the words "anorexic" and "bulimic." When I wrote my dissertation, which was largely on cutting, I drove my advisor nuts because I refused to write the word, "cutter," and instead made my dissertation significantly longer, I am sure, by writing "individuals who engage in self-harm" and similar phrases. So, here's the point: Do you call someone who has cancer, cancer-ic? No, you don't. So, why would someone with anorexia be "an anorexic." The person is not his or her disorder, and in fact, identifying with the disorder is one of the major hurdles to overcome in treatment. So, hearing "anorexic" over and over was very upsetting. This patient did not need to identified as her disorder. She is a person, with a disorder; she is not actually a disorder.
News stories seem to feel such pull to glamorize eating disorders also. Maybe glamorize is not quite the right word. But, they feel the need to show exactly what symptoms the person engages in, his/her weight, etc. All the things that those with eating disorders compete over. So, maybe the news story helped those who know absolutely nothing about EDs understand what behaviors make up an ED, but I was frustrated because I knew those with EDs who were watching the story were being triggered right and left. Some simple research on the part of the reporters would have helped them understand the disorder better, and know what they decided to focus on not only is not unique, but likely triggering to others with the disorder about which they were trying to educate.
So, what could the story have been about instead? How about using this woman's story, without all the details, to present the message that there needs to be greater insurance coverage for treatment? There would have been a lot of benefit to trying to engage people in the fight against insurance companies, or to strengthen laws regarding mental healthy parity. People left that news story knowing what symptoms make up anorexia, and one individual that has the disorder. So much more good could have been done by focusing less on the details, and more on what needs to change within our healthcare system when it comes to eating disorder treatment and coverage.
I want to make it clear I am not criticizing the woman in the piece. She has an eating disorder and deserves access to treatment and, I'm assuming, took the steps she thought could help her get help. I'm criticizing those who were more in the position to treat this story differently, and create greater benefit.
Update: I was just called by the new outlet to come on air live for their follow up story. I refused on principle, and let them know my concerns with their approach to this story. So, hopefully the information I gave them will help change their approach in follow up.
Friday, November 2, 2012
Opinions on weighing
A recent discussion on a professional listserv was regarding whether or not providers weigh patients and communicate their weight to them. At about the same time, a normal weight patient in the process of learning Intuitive Eating commented to me that she felt that being weighed by her dietitian went counter to learning IE, which I thought was an interesting point, so I brought this question to the listserv.
Everywhere I have ever worked has not shown the weights to patients, instead making the treatment team responsible for weights and encouraging patients to not focus on weight, but to instead focus on becoming healthy. Which is what still makes the most sense to me. Weight has recently been such a topic of debate within the field, with of course the "old school way" being to focus likely too much on weight, which has resulted in many problems getting appropriate insurance coverage for EDs. The insurance industry took the height/weight numbers identified in the DSM, and used these to justify terminating treatment ridiculously early. As a result, I believe the weight criteria will be removed for the DSM-V, but don't quote me on that. But then the "new school" seems to, in my opinion, go a little overboard in saying we shouldn't care about patient weights at all, and instead focus solely on physical signs of starvation.
Personally, I think it is more realistic to be in the middle ground. Reality is that weight is one of the more concrete indicators we have to work with in treating eating disorders. But, it certainly is not the be all and end all, since reality is nobody can ever know what is the "right" weight for someone. So, I both track patient weights, through a dietitian or physician, but also ask patients questions that assess for cognitive and physical effects of starvation. I don't think you can do just one or the other because, in my experience, sometimes the cognitive effects don't necessarily change immediately upon the patient seeming to get to a healthy weight, but instead develop over the next little while, while they maintain that healthy weight.
I think most everyone agrees we need to weigh patients who need to gain weight; I saw no debate of that point. But then there's the debate of whether the weight should be shown to the patient. I can see benefits to showing the weight, especially for patients who dramatically overestimate what they weigh or how quickly they are gaining. But I guess I'm not sure why we would show weights for any other reason. To show weights seems, to me, like it perhaps reinforces the message that the weight is important. Though, again, I'm sure there's a middle ground wherein the weight is shown, but also discussed as being not nearly as important as physical and emotional health. I guess I'm just concerned that showing weights could end up taking up more therapeutic time than if the individual just learns to not focus on weight without seeing and reacting to it.
To address my question of weighing in those of normal weight and learning Intuitive Eating, Elyse Resch, one of the authors of Intuitive Eating, did confirm what my patient had said, and argued that patients who are learning IE, should not ever be weighed, as this does propagate the focus on weight and number. But then, we have had patients who want to turn over weighing to us for fear that if their weight is not tracked, they will gain weight and nobody will know. But then others feel shame and guilt even stepping on the scale, perhaps due to things like weigh-ins at Weight Watchers.
So, as you can see, this is proving to be a bit of a confusing topic! As far as I heard on the listserv, nobody has ever actually researched the effect of doing blind vs non-blind weights. So, I thought we should do our own, terribly informal, qualitative research here, and ask for your thoughts on blind vs non-blind weights. Please, comment away!!
Everywhere I have ever worked has not shown the weights to patients, instead making the treatment team responsible for weights and encouraging patients to not focus on weight, but to instead focus on becoming healthy. Which is what still makes the most sense to me. Weight has recently been such a topic of debate within the field, with of course the "old school way" being to focus likely too much on weight, which has resulted in many problems getting appropriate insurance coverage for EDs. The insurance industry took the height/weight numbers identified in the DSM, and used these to justify terminating treatment ridiculously early. As a result, I believe the weight criteria will be removed for the DSM-V, but don't quote me on that. But then the "new school" seems to, in my opinion, go a little overboard in saying we shouldn't care about patient weights at all, and instead focus solely on physical signs of starvation.
Personally, I think it is more realistic to be in the middle ground. Reality is that weight is one of the more concrete indicators we have to work with in treating eating disorders. But, it certainly is not the be all and end all, since reality is nobody can ever know what is the "right" weight for someone. So, I both track patient weights, through a dietitian or physician, but also ask patients questions that assess for cognitive and physical effects of starvation. I don't think you can do just one or the other because, in my experience, sometimes the cognitive effects don't necessarily change immediately upon the patient seeming to get to a healthy weight, but instead develop over the next little while, while they maintain that healthy weight.
I think most everyone agrees we need to weigh patients who need to gain weight; I saw no debate of that point. But then there's the debate of whether the weight should be shown to the patient. I can see benefits to showing the weight, especially for patients who dramatically overestimate what they weigh or how quickly they are gaining. But I guess I'm not sure why we would show weights for any other reason. To show weights seems, to me, like it perhaps reinforces the message that the weight is important. Though, again, I'm sure there's a middle ground wherein the weight is shown, but also discussed as being not nearly as important as physical and emotional health. I guess I'm just concerned that showing weights could end up taking up more therapeutic time than if the individual just learns to not focus on weight without seeing and reacting to it.
To address my question of weighing in those of normal weight and learning Intuitive Eating, Elyse Resch, one of the authors of Intuitive Eating, did confirm what my patient had said, and argued that patients who are learning IE, should not ever be weighed, as this does propagate the focus on weight and number. But then, we have had patients who want to turn over weighing to us for fear that if their weight is not tracked, they will gain weight and nobody will know. But then others feel shame and guilt even stepping on the scale, perhaps due to things like weigh-ins at Weight Watchers.
So, as you can see, this is proving to be a bit of a confusing topic! As far as I heard on the listserv, nobody has ever actually researched the effect of doing blind vs non-blind weights. So, I thought we should do our own, terribly informal, qualitative research here, and ask for your thoughts on blind vs non-blind weights. Please, comment away!!
Tuesday, October 30, 2012
Restricting causes bingeing
I'm really not sure how I made it this far in this blog without more directly addressing this topic. And, I know I have referred to it in a couple other posts, but this is such a key concept that so many people...patients, family, and providers alike....just don't understand. And, fortunately, it's a very simple concept also.
I recently had another provider give me the most brilliantly phrased psychological assessment of a patient. I was blown away by the providers ability to phrase a summary of the patient's treatment, and the psychological explanation for the patient's bingeing, which I will admit was likely right on. There was just one important variable missing for this provider, and in my experience, for many providers, when it comes to helping patient create behavior change around binge eating behaviors.
What this provider was missing was that the patient was restricting all day long, and bingeing at night. And, this is what most people do, in my experience. Dieters do it, and those with eating disorders do it. They tried to make it as long as possible during the day without eating, but then the physiology of all that catches up at night, and the person ends up overeating. And they think this means they have no control, no willpower, that they are weak; and their provider may think it is some emotional trigger that causes this behavior. But, as long as the person is restricting, that should be assumed to be the "cause" of bingeing or overeating. How we explain it to patients is that we must correct the physiology first, and then we'll have a better sense of what is psychological. So, in this case, we see that most bingeing behaviors are corrected by eating more throughout the day, but of course, there are then psychological factors such as stress or anxiety that result in ongoing overeating; that is when therapy really comes into to address those factors.
But if you miss the fact that someone who is binge eating is also restricting (and in our experience, the vast majority do), a provider, or the patient, can end up looking for psychological explanations, and pursuing those routes, only to result in greater frustration that the behavior continues.
Of course, as I have referenced before, the trick is that many who binge eat don't want to stop restricting. They are afraid of weight gain and don't want to take the risk of that happening by eating more during the day. But, in the end, the "math problem" tends to balance out; the amount of calories consumed by eating more during the day is about the same as, or even less then, the amount eaten as a result of restricting and then bingeing. Eating regularly during the day is also of significantly greater benefit to one's metabolism also, whereas restricting can really only result in decreased metabolism. Your body cannot burn what is not there to burn, so it's only option is to burn less.
So, the main thing I would want binge eaters to understand is that their behavior is NOT the result of low motivation, laziness, weakness, lack of willpower, etc. That is the "easy answer," but in my experience, never the right one. No matter how much our society might say it is true. And, to be clear, restricting is also not a sign of strength or willpower, even if it may feel like it for the moment. Treatment is the sign of strength and willpower. I do not work with a single weak person, that is for sure.
I recently had another provider give me the most brilliantly phrased psychological assessment of a patient. I was blown away by the providers ability to phrase a summary of the patient's treatment, and the psychological explanation for the patient's bingeing, which I will admit was likely right on. There was just one important variable missing for this provider, and in my experience, for many providers, when it comes to helping patient create behavior change around binge eating behaviors.
What this provider was missing was that the patient was restricting all day long, and bingeing at night. And, this is what most people do, in my experience. Dieters do it, and those with eating disorders do it. They tried to make it as long as possible during the day without eating, but then the physiology of all that catches up at night, and the person ends up overeating. And they think this means they have no control, no willpower, that they are weak; and their provider may think it is some emotional trigger that causes this behavior. But, as long as the person is restricting, that should be assumed to be the "cause" of bingeing or overeating. How we explain it to patients is that we must correct the physiology first, and then we'll have a better sense of what is psychological. So, in this case, we see that most bingeing behaviors are corrected by eating more throughout the day, but of course, there are then psychological factors such as stress or anxiety that result in ongoing overeating; that is when therapy really comes into to address those factors.
But if you miss the fact that someone who is binge eating is also restricting (and in our experience, the vast majority do), a provider, or the patient, can end up looking for psychological explanations, and pursuing those routes, only to result in greater frustration that the behavior continues.
Of course, as I have referenced before, the trick is that many who binge eat don't want to stop restricting. They are afraid of weight gain and don't want to take the risk of that happening by eating more during the day. But, in the end, the "math problem" tends to balance out; the amount of calories consumed by eating more during the day is about the same as, or even less then, the amount eaten as a result of restricting and then bingeing. Eating regularly during the day is also of significantly greater benefit to one's metabolism also, whereas restricting can really only result in decreased metabolism. Your body cannot burn what is not there to burn, so it's only option is to burn less.
So, the main thing I would want binge eaters to understand is that their behavior is NOT the result of low motivation, laziness, weakness, lack of willpower, etc. That is the "easy answer," but in my experience, never the right one. No matter how much our society might say it is true. And, to be clear, restricting is also not a sign of strength or willpower, even if it may feel like it for the moment. Treatment is the sign of strength and willpower. I do not work with a single weak person, that is for sure.
Friday, October 26, 2012
More on body image
If it is indeed true that body image is one of the last things to change, imagine the experience of going through eating disorder treatment. Patients would, logically, want to feel better about their body so they can feel better about changing it, right? But it just doesn't work that way. So, what patients are asked to do is very hard indeed.
Patients are asked to put their appearance as a lower priority than their health, or their future goals. I wish I knew of a way to make it so they liked their body. And of course there are plenty of messages in our society that if we just change our body, we will be happy, healthier, probably even wealthier. What a misleading message. In reality, focusing on our bodies makes us unhappier and less healthy, both physically and psychologically. But, that simply is not how it seems in the moment.
Families and friends often come in, valiantly trying to rationalize with their loved one about their body. They try and try to convince their loved one that what they see in the mirror is not what is reality, and/or why do they have to care so much about their weight. And this is where it is important to be reminded that eating disorders are not rational diseases, and thus, unfortunately, rationalizing often has little to no benefit, and instead serves to frustrate everyone involved.
So, this bears the question: What do we do instead when our loved one is so upset about her body? Try to remain non-emotional and avoid the frustration. Assume what he/she is saying is what he/she really sees and/or believes, and put yourself in that position. It doesn't mean you agree with what they are saying or thinking about their body, and you can certainly say you do not agree. But, let them see you can understand, as best you can, just how much it hurts to believe what they believe.
Maybe ask them if there is any part of their body they do like; I often jokingly reference the big toe just to make the point that there is maybe some small part of their body they might not hate. And, yes, toenails has been an answer before. What about any part of their body they can value in some way other than appearance. For example, in my experience, many female athletes HATE their legs. They see their muscle as fat, or fear that others think their muscle is fat. But, they often can recognize they also value the strength of their muscular legs.
Also, help your loved one talk about whether they can make anything else more important than their appearance. Are there any situations where they forget, for even a second, about their body? Admittedly, these are often conversations that seem to go better in therapy than at home, so don't become upset if these topics don't seem to help.
Finally, look at yourself and things you perhaps unconsciously say or do. Be aware of whether you, or any other family or friends comment about your own appearance, or anyone else's. Work to change any family patterns around food and weight that unintentionally reinforce an eating disorder. Our society reinforces eating disorders ALL THE TIME, so of course families in our culture do. It's not about blaming the family, or even the culture; it's about understanding what change could help.
Body image concerns are so confusing to those who do not see themselves in such a critical and irrational way. But, coming to understand what your loved one does see can really help you support them in changing it.
Patients are asked to put their appearance as a lower priority than their health, or their future goals. I wish I knew of a way to make it so they liked their body. And of course there are plenty of messages in our society that if we just change our body, we will be happy, healthier, probably even wealthier. What a misleading message. In reality, focusing on our bodies makes us unhappier and less healthy, both physically and psychologically. But, that simply is not how it seems in the moment.
Families and friends often come in, valiantly trying to rationalize with their loved one about their body. They try and try to convince their loved one that what they see in the mirror is not what is reality, and/or why do they have to care so much about their weight. And this is where it is important to be reminded that eating disorders are not rational diseases, and thus, unfortunately, rationalizing often has little to no benefit, and instead serves to frustrate everyone involved.
So, this bears the question: What do we do instead when our loved one is so upset about her body? Try to remain non-emotional and avoid the frustration. Assume what he/she is saying is what he/she really sees and/or believes, and put yourself in that position. It doesn't mean you agree with what they are saying or thinking about their body, and you can certainly say you do not agree. But, let them see you can understand, as best you can, just how much it hurts to believe what they believe.
Maybe ask them if there is any part of their body they do like; I often jokingly reference the big toe just to make the point that there is maybe some small part of their body they might not hate. And, yes, toenails has been an answer before. What about any part of their body they can value in some way other than appearance. For example, in my experience, many female athletes HATE their legs. They see their muscle as fat, or fear that others think their muscle is fat. But, they often can recognize they also value the strength of their muscular legs.
Also, help your loved one talk about whether they can make anything else more important than their appearance. Are there any situations where they forget, for even a second, about their body? Admittedly, these are often conversations that seem to go better in therapy than at home, so don't become upset if these topics don't seem to help.
Finally, look at yourself and things you perhaps unconsciously say or do. Be aware of whether you, or any other family or friends comment about your own appearance, or anyone else's. Work to change any family patterns around food and weight that unintentionally reinforce an eating disorder. Our society reinforces eating disorders ALL THE TIME, so of course families in our culture do. It's not about blaming the family, or even the culture; it's about understanding what change could help.
Body image concerns are so confusing to those who do not see themselves in such a critical and irrational way. But, coming to understand what your loved one does see can really help you support them in changing it.
Tuesday, October 16, 2012
Separating the eating disorder from the person
Patients will come in, and some will joke in an embarrassed way that they sound like they have schizophrenia (though they usually call in multiple personalities). They are able to identify that there's this separate voice in their heads, telling them what to do with food. They do not have schizophrenia. I think Jenni Schaefer, in her book Life Without ED is the first person (that I know of) that really clearly put into words the separation between the person and the ED. And this is such an important distinction. Lock and LeGrange, who have really advocated and research Family Based Treatment (aka Maudsley Method), have also emphasized that parents needs to make this separation in order to best help their child with an eating disorder.
But, this is a hard separation. We all know that. In the moment when the ED is acting up, it is happening in the body of the person you love. And, let's be honest, some moments you want to yell at them, scream at them, shake them, and perhaps wring their necks! (It's okay, you can admit it). So, most parents/loved ones do indeed end up yelling, screaming, and threatening the person they love who has an eating disorder.
But, the patient on the receiving end of all this, kind of has two choices at that point. Okay, three, but #3 is a bit of a huge feat to accomplish.
But, this is a hard separation. We all know that. In the moment when the ED is acting up, it is happening in the body of the person you love. And, let's be honest, some moments you want to yell at them, scream at them, shake them, and perhaps wring their necks! (It's okay, you can admit it). So, most parents/loved ones do indeed end up yelling, screaming, and threatening the person they love who has an eating disorder.
But, the patient on the receiving end of all this, kind of has two choices at that point. Okay, three, but #3 is a bit of a huge feat to accomplish.
- One, they can fight back, and essentially further embody the eating disorder. They can yell and scream and stomp their feet, which only serves to reinforce the idea that he/she, the patient, is setting out to torture those around him/her.
- Two, they can take the anger in, blaming him/herself for being a "bad person," which again, gives the ED more power.
- Three, they could assume the very, very best of their loved ones, be able to understand they really are mad at the disorder, not them, and choose to fight the disorder with their loved one. Sounds great, huh?
I'm a parent, okay stepparent, of a teenager, and I'll easily confess that, at times, strangling her has seemed a viable option. So, there you go, even the psychologist admits that even she cannot do what she is about to say flawlessly. But, in the end, strangling someone doesn't really accomplish much, right? So, what do you do instead?
You separate the disorder from the person. You realize the person is in a battle with that voice inside his/her own head, and doesn't like the battle any more than you do, though some days he/she is more convinced that voice is right than wrong. So, some days, he/she may not join your "team" as much as she might the next day. But, if you can remember it is you and your loved one against a terrible disorder, then hopefully you can each get mad at the disorder. I promise you, the person is also mad at the disorder; it has taken away things that are important to him or her. But, she still is likely to respond to you in anger if you get angry at her. I want to be clear, I am not saying be soft, be lenient, let things slide. Those of you who know me are laughing right now because you KNOW that's not what I mean. Be very hard on that disorder, fight it with all you have. But don't fight the person, fight the disorder. You are more than welcome to despise, hate, want to destroy the disorder. Just as you would if your child had cancer. But, just as you wouldn't yell at your loved one for having cancer, try your hardest not to yell at your loved one with an eating disorder.
The Mask
This is a poem, written by Anonymous, that I used to always read when I provided lectures on eating disorders:
Take a look at my face
What do you see?
A woman who shows you
What she wants you to see.
Hear my spoken words
what do they say?
Only what I want you to hear
It's better that way.
See my ongoing smile
What does it show?
Only a small part of me
That I want you to know.
Hear my witty responses
Do they make you laugh?
That satisfies a small hunger
to be accepted at last.
The feelings I express
Do you think that I"m strong
It's what I need you to think
and again I press on.
If you looked deep in my eyes
It's what I can't let you see
The most incredibly fear
That's strangling me.
If you heard all my thoughts
That I can't let you know
Of shear desperation
That's threatening to show.
If you saw behind the smile
That at this point's painted on
Because my heart's slowly breaking
All security's gone.
My casual wit
A facade nothing more
That once came to ease
Is now such a chore.
If I let you know
Just what makes me tick
I'd lose all control
It's too much of a risk.
So you'll know me best
As who I wish I could be
Someone strong and courageous
really so unlike me.
The poem is sad, but I think accurately represents what those with EDs feel like when trapped in the disorder, partly wanting to hide, and partly wanting their pain to be seen.
However, I must disagree with the last two lines. Fighting an ED requires a ton of strength and courage. Just this morning I watched the internal battle of a young woman who has the "anorexic wish:" Please help me get better without gaining weight. It is anything but weakness that one sees in someone fighting an ED.
Take a look at my face
What do you see?
A woman who shows you
What she wants you to see.
Hear my spoken words
what do they say?
Only what I want you to hear
It's better that way.
See my ongoing smile
What does it show?
Only a small part of me
That I want you to know.
Hear my witty responses
Do they make you laugh?
That satisfies a small hunger
to be accepted at last.
The feelings I express
Do you think that I"m strong
It's what I need you to think
and again I press on.
If you looked deep in my eyes
It's what I can't let you see
The most incredibly fear
That's strangling me.
If you heard all my thoughts
That I can't let you know
Of shear desperation
That's threatening to show.
If you saw behind the smile
That at this point's painted on
Because my heart's slowly breaking
All security's gone.
My casual wit
A facade nothing more
That once came to ease
Is now such a chore.
If I let you know
Just what makes me tick
I'd lose all control
It's too much of a risk.
So you'll know me best
As who I wish I could be
Someone strong and courageous
really so unlike me.
The poem is sad, but I think accurately represents what those with EDs feel like when trapped in the disorder, partly wanting to hide, and partly wanting their pain to be seen.
However, I must disagree with the last two lines. Fighting an ED requires a ton of strength and courage. Just this morning I watched the internal battle of a young woman who has the "anorexic wish:" Please help me get better without gaining weight. It is anything but weakness that one sees in someone fighting an ED.
Saturday, October 13, 2012
Binge eating disorder: the overlooked eating disorder
I was thinking about what to post, and realized I think my own blog represents the ways in which binge eating disorder is overlooked. Sure, so it's not an "official" eating disorder yet. It will be, and regardless, it is something with which many of our patients struggle. It reminds me of the post on competition between the eating disorders. I guess I don't often hear someone with binge eating disorder say they wish they had anorexia, but it wouldn't surprise me if the thought process is there.
I think the vast majority of our binge eating disorder patients don't even recognize their disorder is also fraught with restriction. The typical pattern for binge eating that I see is restriction in two different ways. One, there's the long-term restriction of multiple diets throughout their lives. Then, there's the day-to-day restriction, where they do not eat enough during the day, and then binge at night. But, in my experience, binge eaters look at their own body size and think both that they don't "deserve" the label of an eating disorder (because only the emaciated REALLY have eating disorders), and they cannot possibly restrict. So, at the beginning, it is often a bit of a battle on our parts to help those with BED recognize they are restricting. But they must recognize this as they likely will not stop bingeing if they do not stop restricting.
A couple of themes that have come up with those who binge eat and/or compulsively overeat and, as a result, are at a higher weight. First, they often refuse to go to doctors anymore because, as they say, "I don't need anyone else to tell me I need to lose weight. It's like they think I'm not aware I weigh what I do." Second, almost without fail, these patients have a very limited ability to show any emotion. A few recently have talked about this concept in being "the funny, fat friend." They report feeling pressure to show everyone how funny they can be, seemingly to compensate for their weight.
We have struggled and struggled to start a binge eating group. I may have commented before on the difficult nature of trying to run any type of eating disorder group, given all the comparing and social anxiety. But, my guess is that the shame has been so strongly instilled in those with binge eating disorder, especially those at higher weights, that they just suffer in silence, not wanting to subject themselves to more judgement; even from those who suffer from the same behaviors. I remain optimistic that we will get a binge eating group started. I think it is greatly needed; especially so there can be a place where nobody needs to be the "funny, fat friend."
I think the vast majority of our binge eating disorder patients don't even recognize their disorder is also fraught with restriction. The typical pattern for binge eating that I see is restriction in two different ways. One, there's the long-term restriction of multiple diets throughout their lives. Then, there's the day-to-day restriction, where they do not eat enough during the day, and then binge at night. But, in my experience, binge eaters look at their own body size and think both that they don't "deserve" the label of an eating disorder (because only the emaciated REALLY have eating disorders), and they cannot possibly restrict. So, at the beginning, it is often a bit of a battle on our parts to help those with BED recognize they are restricting. But they must recognize this as they likely will not stop bingeing if they do not stop restricting.
A couple of themes that have come up with those who binge eat and/or compulsively overeat and, as a result, are at a higher weight. First, they often refuse to go to doctors anymore because, as they say, "I don't need anyone else to tell me I need to lose weight. It's like they think I'm not aware I weigh what I do." Second, almost without fail, these patients have a very limited ability to show any emotion. A few recently have talked about this concept in being "the funny, fat friend." They report feeling pressure to show everyone how funny they can be, seemingly to compensate for their weight.
We have struggled and struggled to start a binge eating group. I may have commented before on the difficult nature of trying to run any type of eating disorder group, given all the comparing and social anxiety. But, my guess is that the shame has been so strongly instilled in those with binge eating disorder, especially those at higher weights, that they just suffer in silence, not wanting to subject themselves to more judgement; even from those who suffer from the same behaviors. I remain optimistic that we will get a binge eating group started. I think it is greatly needed; especially so there can be a place where nobody needs to be the "funny, fat friend."
Wednesday, October 10, 2012
Ohhh, body image
Wow, body image. Such a difficult topic, in my opinion. I do think it is the very last thing to change in an eating disorder, which is really quite unfair. At the same time, I think there can be significant improvement in body image, both for physiological and psychological reasons, as ED behaviors stop.
Physiologically, we know from the Keys Study that body image concerns can be created from starvation alone. In short, the Keys Study showed that when they starved down totally normal men (this was for a completely non-ED related study, by the way), they developed dissatisfaction with their appearance. The men did not have EDs, but began to illustrate a number of behaviors we typically think as being caused by the ED. This study is the main thing that has illustrated that starvation must be addressed prior to, or at least at the same time as, working on the psychology of the ED, because many ED thoughts and feelings can improve with appropriate food intake and weight. In these men, weight gain alone corrected the body image concerns.
I have a colleague who developed cancer, and had to have chemotherapy. She lost a significant amount of weight, and one day, she looked at me and said she finally understood the body image part of eating disorders. She told me that, before she got cancer, she was satisfied with her appearance and weight. However, after losing weight, she found herself reticent to regain weight, though recognized this made no sense. So, this example also demonstrates how starvation alone causes body image concerns.
But, let me tell you, trying to convince a currently low weight patient that they will FEEL BETTER about their body as they gain weight....that's a pretty hard sell. And, it's not that they will LOVE their body. I have come to describe it this way: You will feel better about your body at that weight then you think you will at this weight. A confusing concept.
The other thing I noticed in working with patients with binge eating disorder was that, once they stopped bingeing, even when their weight stayed the same, they reported improved body image. I think this makes sense, because who can feel good about their body when they are subjecting themselves to any ED symptom.
So, how do I treat body image? Well, I guess I don't really. In those who need to gain weight, I guess I don't much see the benefit. As I explain to them, if I help them accept their weight during weight gain, they just have to keep reaccepting their weight. I think that would be maddening. I certainly know there is research evidence that some body image approaches help, but I guess I'm just not convinced they help enough, and instead may increase focus on one's body.
I think what has impacted me the most was one group I ran in a treatment center. I had asked the group members what they wanted to talk about, and they got me; they wanted to talk about body image. Aack! Somewhere in that group, I spit out a sentence I didn't think was of much consequence. I told the group members my personal approach to body image. It came out something like this:
Sometimes, I don't like what I see in the mirror in the morning; but, then I look at myself, say, "I
have (bleeeep) to do," and head in to work to treat eating disorders.
My point with this was simple; that passions, goals, wants, interests, can outweigh what is seen in the mirror. If I stood there in the mirror and focused on how I looked, I would lose time doing my passion.
Now, I thought this was just one of those random sentences that comes out of my mouth. I was shocked when patient after patient came up to me over the next few months, saying this one random sentence really changed their view of body image. So, I guess that has always been my focus. Figure out what is more important than the image you see in the mirror. Sure, there are other things you can do....don't body check, pick out parts of your body you do like or value, stop the critical thoughts. But, more so, figure out what is more important....your appearance, or what you want to do with your life?
What things have helped you with body image concerns?
Physiologically, we know from the Keys Study that body image concerns can be created from starvation alone. In short, the Keys Study showed that when they starved down totally normal men (this was for a completely non-ED related study, by the way), they developed dissatisfaction with their appearance. The men did not have EDs, but began to illustrate a number of behaviors we typically think as being caused by the ED. This study is the main thing that has illustrated that starvation must be addressed prior to, or at least at the same time as, working on the psychology of the ED, because many ED thoughts and feelings can improve with appropriate food intake and weight. In these men, weight gain alone corrected the body image concerns.
I have a colleague who developed cancer, and had to have chemotherapy. She lost a significant amount of weight, and one day, she looked at me and said she finally understood the body image part of eating disorders. She told me that, before she got cancer, she was satisfied with her appearance and weight. However, after losing weight, she found herself reticent to regain weight, though recognized this made no sense. So, this example also demonstrates how starvation alone causes body image concerns.
But, let me tell you, trying to convince a currently low weight patient that they will FEEL BETTER about their body as they gain weight....that's a pretty hard sell. And, it's not that they will LOVE their body. I have come to describe it this way: You will feel better about your body at that weight then you think you will at this weight. A confusing concept.
The other thing I noticed in working with patients with binge eating disorder was that, once they stopped bingeing, even when their weight stayed the same, they reported improved body image. I think this makes sense, because who can feel good about their body when they are subjecting themselves to any ED symptom.
So, how do I treat body image? Well, I guess I don't really. In those who need to gain weight, I guess I don't much see the benefit. As I explain to them, if I help them accept their weight during weight gain, they just have to keep reaccepting their weight. I think that would be maddening. I certainly know there is research evidence that some body image approaches help, but I guess I'm just not convinced they help enough, and instead may increase focus on one's body.
I think what has impacted me the most was one group I ran in a treatment center. I had asked the group members what they wanted to talk about, and they got me; they wanted to talk about body image. Aack! Somewhere in that group, I spit out a sentence I didn't think was of much consequence. I told the group members my personal approach to body image. It came out something like this:
Sometimes, I don't like what I see in the mirror in the morning; but, then I look at myself, say, "I
have (bleeeep) to do," and head in to work to treat eating disorders.
My point with this was simple; that passions, goals, wants, interests, can outweigh what is seen in the mirror. If I stood there in the mirror and focused on how I looked, I would lose time doing my passion.
Now, I thought this was just one of those random sentences that comes out of my mouth. I was shocked when patient after patient came up to me over the next few months, saying this one random sentence really changed their view of body image. So, I guess that has always been my focus. Figure out what is more important than the image you see in the mirror. Sure, there are other things you can do....don't body check, pick out parts of your body you do like or value, stop the critical thoughts. But, more so, figure out what is more important....your appearance, or what you want to do with your life?
What things have helped you with body image concerns?
Thursday, October 4, 2012
Insurance coverage for ED treatment
I see many an article, even a blog post, on insurance coverage for eating disorders and how poorly treatment is covered. I could write probably a more professional, appropriate post on this, but honestly, I'm not in the mood for such niceties. Below is the reality of being an eating disorder provider:
There's a young woman I care deeply for who is soon likely to die of her eating disorder. Now, certainly in the past she has had treatment and she has relapsed by making choices that were not consistent with her recovery. But, regardless, right now, her eating disorder is severe. Her body is shutting down, and she is going to die without expert intervention. She is currently in setting that is not able to manage her ED symptoms. Her insurance company is taking the "one program fits all approach" and refusing to give her any options for a treatment setting.
Mind you, this young woman is willing to go to treatment, she has signed herself into the current setting, she has remained in treatment without walking out. She is voluntary, and she is begging her insurance for options. The insurance company has heard from me, the patient, the family, the current setting, and we are all singing the same tune: Send this young woman to Program X, a program that is not that far away. They were supposed to have an answer last week, yet this week, she remains without any options, dying in her current setting.
I am irate. To worsen the story, this is the SECOND insurance company I have had to battle in this way for this patient. The previous company said, "She's a terminal case. She should just go to jail; that is a better setting for her." They refused coverage, I fought them. Let's just say they don't like me much anymore and I'm no longer authorized to see their ED patients. I will fight this second insurance company the same way. No amount of money from an insurance company will stop me from standing up to them to try to save this young woman's life.
I witness the emotional detachment others can demonstrate in these situations. Clearly, the insurance company is not seeing this young woman as a person. But, dammit, I know this young woman, she is not just a number, a paycheck, someone who chose this disorder. Until insurance companies, and even non-specialized providers better understand these disorders, we will lose patients. Insurance companies should not "be in bed" with one specific program and refuse to authorize other programs; that is just wrong. Not every patient will like me as his/her therapist, so there are multiple therapists to choose from; so why would they assume one program can serve all their members with eating disorders. This all makes me so angry. I know this young woman, and she does not deserve to die as a result of a breakdown of this system. She deserves one more shot at expert treatment. She deserve me continuing to fight, so I will.
At what point will people....providers, insurance companies, patients themselves....understand these disorders are lethal. They are not to be toyed with, brushed off, denied.
Fight your insurance companies. Hit them with more paper and more phone calls than they know what to do with. They are trying to wait you out, thinking you will back down; don't let it happen. Yes, they are a business, so they must be about the bottom line. But they also are a service industry, and they are serving you. You are paying their salaries. So, fight them. Please.
There's a young woman I care deeply for who is soon likely to die of her eating disorder. Now, certainly in the past she has had treatment and she has relapsed by making choices that were not consistent with her recovery. But, regardless, right now, her eating disorder is severe. Her body is shutting down, and she is going to die without expert intervention. She is currently in setting that is not able to manage her ED symptoms. Her insurance company is taking the "one program fits all approach" and refusing to give her any options for a treatment setting.
Mind you, this young woman is willing to go to treatment, she has signed herself into the current setting, she has remained in treatment without walking out. She is voluntary, and she is begging her insurance for options. The insurance company has heard from me, the patient, the family, the current setting, and we are all singing the same tune: Send this young woman to Program X, a program that is not that far away. They were supposed to have an answer last week, yet this week, she remains without any options, dying in her current setting.
I am irate. To worsen the story, this is the SECOND insurance company I have had to battle in this way for this patient. The previous company said, "She's a terminal case. She should just go to jail; that is a better setting for her." They refused coverage, I fought them. Let's just say they don't like me much anymore and I'm no longer authorized to see their ED patients. I will fight this second insurance company the same way. No amount of money from an insurance company will stop me from standing up to them to try to save this young woman's life.
I witness the emotional detachment others can demonstrate in these situations. Clearly, the insurance company is not seeing this young woman as a person. But, dammit, I know this young woman, she is not just a number, a paycheck, someone who chose this disorder. Until insurance companies, and even non-specialized providers better understand these disorders, we will lose patients. Insurance companies should not "be in bed" with one specific program and refuse to authorize other programs; that is just wrong. Not every patient will like me as his/her therapist, so there are multiple therapists to choose from; so why would they assume one program can serve all their members with eating disorders. This all makes me so angry. I know this young woman, and she does not deserve to die as a result of a breakdown of this system. She deserves one more shot at expert treatment. She deserve me continuing to fight, so I will.
At what point will people....providers, insurance companies, patients themselves....understand these disorders are lethal. They are not to be toyed with, brushed off, denied.
Fight your insurance companies. Hit them with more paper and more phone calls than they know what to do with. They are trying to wait you out, thinking you will back down; don't let it happen. Yes, they are a business, so they must be about the bottom line. But they also are a service industry, and they are serving you. You are paying their salaries. So, fight them. Please.
Wednesday, October 3, 2012
The "perfect patient"
Eating disorder treatment presents with a lot of ironies. They are often disorders of perfection, yet treatment sometimes demands perfection to save the person's life. For example, you need to eat exactly this, nothing more, nothing less, to make sure that we can keep you safe and out of the hospital. Ironic, huh? Never mind that the eating disorder is about over-focus on food and weight, yet what must (good) treatment focus on initially? Food and weight. I'm not sure there could be a more ironic field. Well, I guess sometimes in medicine, a similar thing happens. With cancer; here, take this lethal medication in an effort to save your life. Let's kill off all your body's defenses so it can defend itself better. So, I guess it's not just eating disorders, but it certainly is not the norm.
So, if eating disorders are about perfection, and some level of precision is needed at times during the process, what do you do with the "perfect patient?" These are the patients who come in and they want help on some level, but more so, perhaps, they want you to like them, accept them, approve of them. So, they tell you what they think you want to hear. Often times, they actually do the behaviors perfectly. For instance, they follow their meal plan perfectly, but they are not telling you that it is killing them inside. The outcome, in my experience, is that they gain weight, for example, or they stop bingeing and purging, or they stop whatever ED symptom, but the psychological parts of the disorder go unaddressed because they are showing you they are perfect, and are handling things perfectly. They are at high risk of relapse, as a result. And then they can't tell you about the relapse, because a relapse isn't perfect.
On the surface, it sure is nice to have a compliant patient. What a relief, right? Well, not so much. Because eating disorders are terribly painful diseases; they are hell to live with and to overcome. So, the process should not look perfect. Now, in that, I'm not saying that we should expect and accept non-compliance, because that won't help anything either. No, I'm saying that we need compliance, but honesty about horribly painful and difficult that compliance is. That is treatment. That is recovery. If your patient or your loved one is smiling at you about recovery from his/her ED, look deeper. Help him/her to talk about how it really feels to do what needs to be done in order to recover. In doing that, he/she relearns how to talk about all that he/she used her ED to avoid. As the ability to communicate returns, the need for the eating disorder decreases.
That is treatment. That is recovery.
So, if eating disorders are about perfection, and some level of precision is needed at times during the process, what do you do with the "perfect patient?" These are the patients who come in and they want help on some level, but more so, perhaps, they want you to like them, accept them, approve of them. So, they tell you what they think you want to hear. Often times, they actually do the behaviors perfectly. For instance, they follow their meal plan perfectly, but they are not telling you that it is killing them inside. The outcome, in my experience, is that they gain weight, for example, or they stop bingeing and purging, or they stop whatever ED symptom, but the psychological parts of the disorder go unaddressed because they are showing you they are perfect, and are handling things perfectly. They are at high risk of relapse, as a result. And then they can't tell you about the relapse, because a relapse isn't perfect.
On the surface, it sure is nice to have a compliant patient. What a relief, right? Well, not so much. Because eating disorders are terribly painful diseases; they are hell to live with and to overcome. So, the process should not look perfect. Now, in that, I'm not saying that we should expect and accept non-compliance, because that won't help anything either. No, I'm saying that we need compliance, but honesty about horribly painful and difficult that compliance is. That is treatment. That is recovery. If your patient or your loved one is smiling at you about recovery from his/her ED, look deeper. Help him/her to talk about how it really feels to do what needs to be done in order to recover. In doing that, he/she relearns how to talk about all that he/she used her ED to avoid. As the ability to communicate returns, the need for the eating disorder decreases.
That is treatment. That is recovery.
Tuesday, October 2, 2012
Involving families in eating disorder treatment
Brie asked that I address the topic of involving families in the treatment process, especially for adult patients. I think this is something we do that is maybe a bit more unique. But, I also am somewhat blown away by the number of providers who treat children and adolescents, with and without eating disorders, without including the family. I don't see how that make sense. Therapy is one hour out of a week that has, ummm, 168 hours, I think. I just don't see how therapy alone will be powerful enough to override an eating disorder that resides in the patient's mind each of those 168 hours.
When it comes to involving family in an adult's treatment, however, there reasonably can be some hesitation. After all, adults don't want to feel like they have been rewinded to childhood or adolescence, and have to answer to Mom and Dad; this is fair! But, again, this disorder is lodged in the mind of the patient ALL THE TIME. It damages the individual's brain, and thus his or her thought processes, and rational thought suffers as a result of damage to the frontal lobe. I often speak of the vortex that exists right at my office door. When patients sit on my couch, it makes sense to give up their ED, stop the behaviors, and choose health. But, they hit that vortex, and get slammed by the world, and suddenly, that motivation and desire can wane.
So, here's where family and friends come in. But, it is key that the adult patient drive the family/friend involvement. They need to be able to tell their family/friends what they can do to help, and give them permission to say the difficult things the ED does not want to hear. Many patients will choose this path because it is the intervention that comes immediately prior to hospitalization; so, for those who do not want to be hospitalized, a good number will choose this alternative.
And, really, I think what most of us probably want is our family/friends' support anyway. When you have an ED, you tend to lose the ability to communicate as well, so it is harder to ask for that help. I have seen many patients feel great relief from being able to address their ED with those they care about in a safe environment, where a therapist can help the family to understand that the disorder is not rational and that, often, their gut reactions are not what is most helpful to the patient. I can write more on that at a later time.
Now, selfishly, as a provider, I will say that it is also helpful to have family and friends involved to help avoid unintentional undermining of what we are trying to do. If you think of the patient as having this totally separate voice in their head, the voice of the ED, and then the providers are trying to challenge the disorder; well, we are not always EXACTLY correctly quoted by the time the patient makes it home. In addition, with families being on the front lines of the battle against the disorder, they sometimes are more likely to try to negotiate with the disorder, perhaps saying a lower weight is reasonable, or that the patient doesn't need as much support as the treatment team recommends. If the family/friends are involved in the treatment itself, it provides an avenue where they can ask why we do what we do, and hopefully then feel more able to support our recommendations.
In short, EDs are terrible disorders that cause so much damage. The more people who can help treat them, the better. Families used to be banned from treatment because psychology LOVED blaming parents. Now, I think we all need to recognize that blaming parents has no benefit, but involving them in helping, when they are willing, can have incredible power.
When it comes to involving family in an adult's treatment, however, there reasonably can be some hesitation. After all, adults don't want to feel like they have been rewinded to childhood or adolescence, and have to answer to Mom and Dad; this is fair! But, again, this disorder is lodged in the mind of the patient ALL THE TIME. It damages the individual's brain, and thus his or her thought processes, and rational thought suffers as a result of damage to the frontal lobe. I often speak of the vortex that exists right at my office door. When patients sit on my couch, it makes sense to give up their ED, stop the behaviors, and choose health. But, they hit that vortex, and get slammed by the world, and suddenly, that motivation and desire can wane.
So, here's where family and friends come in. But, it is key that the adult patient drive the family/friend involvement. They need to be able to tell their family/friends what they can do to help, and give them permission to say the difficult things the ED does not want to hear. Many patients will choose this path because it is the intervention that comes immediately prior to hospitalization; so, for those who do not want to be hospitalized, a good number will choose this alternative.
And, really, I think what most of us probably want is our family/friends' support anyway. When you have an ED, you tend to lose the ability to communicate as well, so it is harder to ask for that help. I have seen many patients feel great relief from being able to address their ED with those they care about in a safe environment, where a therapist can help the family to understand that the disorder is not rational and that, often, their gut reactions are not what is most helpful to the patient. I can write more on that at a later time.
Now, selfishly, as a provider, I will say that it is also helpful to have family and friends involved to help avoid unintentional undermining of what we are trying to do. If you think of the patient as having this totally separate voice in their head, the voice of the ED, and then the providers are trying to challenge the disorder; well, we are not always EXACTLY correctly quoted by the time the patient makes it home. In addition, with families being on the front lines of the battle against the disorder, they sometimes are more likely to try to negotiate with the disorder, perhaps saying a lower weight is reasonable, or that the patient doesn't need as much support as the treatment team recommends. If the family/friends are involved in the treatment itself, it provides an avenue where they can ask why we do what we do, and hopefully then feel more able to support our recommendations.
In short, EDs are terrible disorders that cause so much damage. The more people who can help treat them, the better. Families used to be banned from treatment because psychology LOVED blaming parents. Now, I think we all need to recognize that blaming parents has no benefit, but involving them in helping, when they are willing, can have incredible power.
Competition among the eating disorders
Reader Krista brought up this point of comparisons between those with eating disorders, and asked if she is the only one seeing that anorexia is glorified while bulimia is looked down upon. And, no, Krista, you are not the only one seeing this. I see it all the time and take a number of steps to try to avoid this in the group that I run, though certainly I understand I cannot change what is going on in each patient's mind.
I think the root of this is that our society glamorized dietary restriction. Which frustrates me to know end because I am very aware eating disorders are lethal; the most lethal of all psychiatric diagnoses. So, to have such a lethal behavior glamorized certainly shows the level of ignorance, but also just really irritates me, honestly! Those who restrict, whether in an ED or not, are seen as having control, willpower, strength, and power. Now, those with eating disorders generally know nothing could be farther from the truth. Sure, engaging in an ED can create a feeling of power and control at times, but most realize having an ED actually is a feeling of being out of control and powerless against the voice in your head.
Bingeing or bingeing and purging is simply not seen as as glamorous, so restricting is seen as the symptom of choice. In reality, those who binge and purge, the vast majority of the time, also restrict; that's the physiology that sets up the binge. But it is interesting how often those who binge and purge, and binge without purging, overlook their restricting because they feel such intense shame around the bingeing behavior.
Something that I think is also related is this concept of those with low weight eating disorders being able to use their body, their disorder, to communicate. Those without the low weight, I think, do not necessarily have that way of showing others that they need help, and so I think, for some, they may want that lower weight so that they are less invisible, ironically. This is just a thought on my part, nothing I have seen confirmed by research findings.
I think the root of this is that our society glamorized dietary restriction. Which frustrates me to know end because I am very aware eating disorders are lethal; the most lethal of all psychiatric diagnoses. So, to have such a lethal behavior glamorized certainly shows the level of ignorance, but also just really irritates me, honestly! Those who restrict, whether in an ED or not, are seen as having control, willpower, strength, and power. Now, those with eating disorders generally know nothing could be farther from the truth. Sure, engaging in an ED can create a feeling of power and control at times, but most realize having an ED actually is a feeling of being out of control and powerless against the voice in your head.
Bingeing or bingeing and purging is simply not seen as as glamorous, so restricting is seen as the symptom of choice. In reality, those who binge and purge, the vast majority of the time, also restrict; that's the physiology that sets up the binge. But it is interesting how often those who binge and purge, and binge without purging, overlook their restricting because they feel such intense shame around the bingeing behavior.
Something that I think is also related is this concept of those with low weight eating disorders being able to use their body, their disorder, to communicate. Those without the low weight, I think, do not necessarily have that way of showing others that they need help, and so I think, for some, they may want that lower weight so that they are less invisible, ironically. This is just a thought on my part, nothing I have seen confirmed by research findings.
Monday, September 24, 2012
Ambivalence
A topic I have been talking to people about quite a bit recently is that of ambivalence. Outpatient eating disorder treatment is an interesting animal. Most everyone who walks through my doors is wanting treatment; it is only the occasional adolescent that is brought in against his/her will. However, in spite of this, many patients present as very ambivalent. They come in for treatment, and of course pay for it, but they don't necessarily follow what we recommend. So, from the total rational perspective, they are wasting their money, right?
But that's the tricky thing with eating disorders. As I tell patients, the "psychobabble" word is ego-syntonic. I think I have mentioned this before. But, in short, eating disorders serve a number of functions for the patient, so whereas on some level they want to get rid of their eating disorder, on another level, they really don't want to.
So, it is interesting to figure out how to challenge the ambivalence and point it out, without being somewhat offensive, perhaps. Fortunately, because the majority of patients we treat are motivated on some level for treatment, simply identifying the ambivalence is sufficient to break through it.
We can all talk endlessly, probably, about why one should not have an eating disorder. I think the more important question is this.....why is it "good" to have an ED? How does it "help" you?
Also, thanks to you who are still reading. It's been a rough couple weeks. I'll try to get more on track with posting, however. I still would love topic suggestions; sometimes my brain just can't come up with enough ideas!
But that's the tricky thing with eating disorders. As I tell patients, the "psychobabble" word is ego-syntonic. I think I have mentioned this before. But, in short, eating disorders serve a number of functions for the patient, so whereas on some level they want to get rid of their eating disorder, on another level, they really don't want to.
So, it is interesting to figure out how to challenge the ambivalence and point it out, without being somewhat offensive, perhaps. Fortunately, because the majority of patients we treat are motivated on some level for treatment, simply identifying the ambivalence is sufficient to break through it.
We can all talk endlessly, probably, about why one should not have an eating disorder. I think the more important question is this.....why is it "good" to have an ED? How does it "help" you?
Also, thanks to you who are still reading. It's been a rough couple weeks. I'll try to get more on track with posting, however. I still would love topic suggestions; sometimes my brain just can't come up with enough ideas!
Wednesday, August 29, 2012
How do you define recovery?
So, of course, the question is: How do you define recovery for yourself?
Monday, August 27, 2012
Dieting causes obesity?
There are things that, in any field, because you are in it, you know it well. And then you think everyone else knows what you know, so of course they will follow it. But, then, in my case, my partner reminds me not everyone thinks the way we do about all this food, weight and exercise stuff. Which is kind of disappointing, you know.
 So, what we in this field know well is DIETING DOESN'T WORK! Oh, don't you worry, it has been researched to death. And that research resoundingly supports the understanding that 95-98% of diets will fail. Will you lose weight initially? Sure, some will, and they might even keep the weight off for a bit. But what the dieting industry leaves out of their marketing material is that 95-98% of people will regain the weight, and a good number of those will actually add 10% to their previous weight. Which, as you can imagine, reinforces starting another diet where they again regain the weight plus 10%. Surely you can see where this is going, right? People diet and actually gain weight! I was first introduced to this concept in my training in about 2002, and it shocked me. I thought, "You mean, in reality, dieting is a major cause of obesity?" Now, am I going to take the time to back up that claim here with research? No, I'm not. (I'm kinda lazy.) I throw it out as more of a discussion piece. But it certainly interesting how weights in the US have increased IN SPITE OF the proliferation of diets. Hmmmmm.
So, what we in this field know well is DIETING DOESN'T WORK! Oh, don't you worry, it has been researched to death. And that research resoundingly supports the understanding that 95-98% of diets will fail. Will you lose weight initially? Sure, some will, and they might even keep the weight off for a bit. But what the dieting industry leaves out of their marketing material is that 95-98% of people will regain the weight, and a good number of those will actually add 10% to their previous weight. Which, as you can imagine, reinforces starting another diet where they again regain the weight plus 10%. Surely you can see where this is going, right? People diet and actually gain weight! I was first introduced to this concept in my training in about 2002, and it shocked me. I thought, "You mean, in reality, dieting is a major cause of obesity?" Now, am I going to take the time to back up that claim here with research? No, I'm not. (I'm kinda lazy.) I throw it out as more of a discussion piece. But it certainly interesting how weights in the US have increased IN SPITE OF the proliferation of diets. Hmmmmm.
 What got me on this kick today was yet another high school acquaintance posting on Facebook how they are going to do something to lose weight. And, really, I don't know if it is the next fad diet, or perhaps worse, weight loss surgery. But each time this happens, I really want to contact these people who I have not spoken to in, uhhh, 19 years, and provide all the information we in this field know that goes counter to the diet industry. I mean, the diet industry has billions of dollars. The eating disorder field? Ahhh, not much. So, we will never be able to counteract the number of messages put out there by the dieting industry. And, that is frustrating.
What got me on this kick today was yet another high school acquaintance posting on Facebook how they are going to do something to lose weight. And, really, I don't know if it is the next fad diet, or perhaps worse, weight loss surgery. But each time this happens, I really want to contact these people who I have not spoken to in, uhhh, 19 years, and provide all the information we in this field know that goes counter to the diet industry. I mean, the diet industry has billions of dollars. The eating disorder field? Ahhh, not much. So, we will never be able to counteract the number of messages put out there by the dieting industry. And, that is frustrating.
But, if I did think it was advisable to contact each of the high school classmates, I would encourage them to work with a therapist to see if any ED behaviors underlie their weight problems. And to see a dietitian who can help them with Intuitive Eating, rather than just another diet. And tackling weight loss surgery is for another day, but these two recommendations (as long as the person sees actual eating disorder treatment experts) would address most concerns about weight loss surgery as well.
 But, alas, most people don't want to hear diets don't work. Until they have done enough of them that they cannot stand it for one more moment, and then many will open their minds to Intuitive Eating. And the dieting cycle and finally end.
But, alas, most people don't want to hear diets don't work. Until they have done enough of them that they cannot stand it for one more moment, and then many will open their minds to Intuitive Eating. And the dieting cycle and finally end.
But, if I did think it was advisable to contact each of the high school classmates, I would encourage them to work with a therapist to see if any ED behaviors underlie their weight problems. And to see a dietitian who can help them with Intuitive Eating, rather than just another diet. And tackling weight loss surgery is for another day, but these two recommendations (as long as the person sees actual eating disorder treatment experts) would address most concerns about weight loss surgery as well.
Thursday, August 23, 2012
High expectations
Because we know the impact of the eating disorder symptoms on the body, mood, functioning, social interaction, etc., we set terminating the symptoms as our initial primary goal. As a therapist, I am aware that trying to do therapy with someone in the midst of ED behaviors is of very limited benefit. One way to think about it is this: If you have an ED, how well do you remember your first, or probably even first few, therapy appointments. In the moment, you felt really with it and like you were fully functioning, and you likely even seemed to your therapist like you were totally with them, but reality is that very few patients remember those initial sessions. So, therapists can walk out thinking they just did excellent therapy but sadly, their therapeutic interaction had little effect because the physiological impact of EDs is so profound.
Dietary sessions are of course focused on ending ED symptoms, but in our model, so is therapy. The best way I can summarize it for patients, and now for you, is:
"Trying to do therapy with someone engaging in eating disorder symptoms is about as
effective as trying to do therapy with an alcoholic in a bar."
Imagine, I ask the inebriated alcoholic how he feels. Riiiiiight. How can therapy be done in that situation; the substance is masking the person's emotions. Same for an eating disorder.
And, I'll confess, I enjoy this second of stage much better than the first stage too.
Wednesday, August 22, 2012
Removing permission to purge
A couple years ago, admittedly a little further along in treating eating disorders than probably ideal, I noticed something. I noticed that when patients with bulimia talk about their symptoms, they would view bingeing and purging as essentially one symptom. And, so, for too long, I too responded as if they were one. When they are one symptom, though, bulimia is incredibly hard to treat. It seemed it was too much to give up both bingeing and purging at one time, and progress seemed to happen slowly.
Then, one day, it occurred to me that they were two separate symptoms, and should be treated as such. And, in that session, I finally realized that purging "allowed" bingeing to happen. As long as the person had "an out" (please do not read this as saying people WANT to purge, that is not my point) with purging, they were "more able" to binge. So, I started with that one patient and talked to her about the possibility of "removing the permission to purge." We talked about how, if she were to no longer allow herself to purge, would she binge? And she admitted that, without purging as an option, she would not be as likely to binge.
So, we moved forward with this concept of "removing the permission to purge," and sure enough, she first stopped purging, and shortly thereafter, stopped bingeing. Now, as this happened, we of course had to deal with all the underlying emotions and thoughts that came up as those ED symptoms were terminated; I make it sound simple here, but it is anything but, I know. But there seemed to be a lot of power in the concept of "removing the permission to purge."
Since, I have introduced this concept to each patient I work with who engages in bingeing and purging. And, as with many things I propose, patients first look at me like I have grown a second head and most certainly lost my mind, but as we talk about the rationale, they eventually become willing to give it a try. It would be ideal if refusing purging meant one never binged again, but that simply isn't the case most of the time. Most patients have been in the position of having to "sit with" a binge, but time and again, that sitting through a binge without purging has created enough of a negative experience that the patient's bingeing decreases dramatically, if it doesn't stop completely. Patients talk about feeling more in control, more confident, and feeling less pull from the eating disorder symptoms.
Of course, once the symptoms stop, the real therapy begins, so they are far from cured. But as I will discuss in another post, the symptoms must stop first for the deeper work to begin.
So, consider it....what impact would it have on your eating disorder if you "removed the permission to purge?"
Then, one day, it occurred to me that they were two separate symptoms, and should be treated as such. And, in that session, I finally realized that purging "allowed" bingeing to happen. As long as the person had "an out" (please do not read this as saying people WANT to purge, that is not my point) with purging, they were "more able" to binge. So, I started with that one patient and talked to her about the possibility of "removing the permission to purge." We talked about how, if she were to no longer allow herself to purge, would she binge? And she admitted that, without purging as an option, she would not be as likely to binge.
So, we moved forward with this concept of "removing the permission to purge," and sure enough, she first stopped purging, and shortly thereafter, stopped bingeing. Now, as this happened, we of course had to deal with all the underlying emotions and thoughts that came up as those ED symptoms were terminated; I make it sound simple here, but it is anything but, I know. But there seemed to be a lot of power in the concept of "removing the permission to purge."
Since, I have introduced this concept to each patient I work with who engages in bingeing and purging. And, as with many things I propose, patients first look at me like I have grown a second head and most certainly lost my mind, but as we talk about the rationale, they eventually become willing to give it a try. It would be ideal if refusing purging meant one never binged again, but that simply isn't the case most of the time. Most patients have been in the position of having to "sit with" a binge, but time and again, that sitting through a binge without purging has created enough of a negative experience that the patient's bingeing decreases dramatically, if it doesn't stop completely. Patients talk about feeling more in control, more confident, and feeling less pull from the eating disorder symptoms.
Of course, once the symptoms stop, the real therapy begins, so they are far from cured. But as I will discuss in another post, the symptoms must stop first for the deeper work to begin.
So, consider it....what impact would it have on your eating disorder if you "removed the permission to purge?"
Tuesday, August 21, 2012
Stumped
I'm thinking more seriously about writing a book on ED treatment, which of course would be an incredibly difficult endeavor, and then there's the reality that there are so many ED books out there. But I really love helping others learn more about treating EDs. Not that I/we have all the answers, but I think we do have a lot to share. I guess for now, I will just have to research the publishing world to see if I have the guts to enter it.
In short, I wonder if the type of book I would want to write is really wanted, or would be very respected. It is very hard to know, and I'd really like to avoid that whole rejection thing! Yep, I prefer to avoid rejection also; don't we all?
I dunno, are there any topics you'd like to hear about? I'm open to about anything....as long as I don't have to do research, apparently!
Monday, August 20, 2012
EDs as a form of communication
Of course, eating disorder 101 is "it's not about the food." Oh, it seems like it is about the food, and one really good way to irritate a patient in the midst of an eating disorder is often to tell them that, in reality, their eating disorder is not about the food.
 I have gotten many a nasty look and deep sigh in response to that one! But I persist on my statement, much to the client's chagrin.
I have gotten many a nasty look and deep sigh in response to that one! But I persist on my statement, much to the client's chagrin.
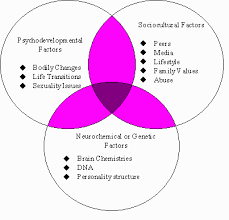 Eating disorder 101, part two, is that very few people will ever know "why" they have an eating disorder. In my 10 years of doing this, and hundreds of patients, I can now say I "know why" a whopping two patients have their eating disorder. For the other hundreds, well, there are just too many reasons. And, reasonably so, most people, and their families want to know why. But, reality is, it is a combination of a number of factors, some genetic and some environmental, and we can almost never identify the why.
Eating disorder 101, part two, is that very few people will ever know "why" they have an eating disorder. In my 10 years of doing this, and hundreds of patients, I can now say I "know why" a whopping two patients have their eating disorder. For the other hundreds, well, there are just too many reasons. And, reasonably so, most people, and their families want to know why. But, reality is, it is a combination of a number of factors, some genetic and some environmental, and we can almost never identify the why.
So, that leaves us with the present reasons for the ED, what needs the ED meets. And even those are numerous, so today I am going to focus on just one: Eating disorders as a form of communication.
 Many individuals with eating disorders struggle to put words to their feelings. Add to that their social isolation and tendency to keep others at a distance, and very rarely will you find an ED patient with a strong social support network with whom they talk openly. They have often lost the ability to walk up to someone and say, "I'm really sad about....," or "I'm so mad that you....."
Many individuals with eating disorders struggle to put words to their feelings. Add to that their social isolation and tendency to keep others at a distance, and very rarely will you find an ED patient with a strong social support network with whom they talk openly. They have often lost the ability to walk up to someone and say, "I'm really sad about....," or "I'm so mad that you....."
In comes the eating disorder. They can use their body to communicate how they feel. So, as their body size decreases or increases, they might be trying to say something that they cannot find the words for. (Note, this is different than that accusation of eating disorders being "attention-seeking." Yes, they are hoping someone will notice and help, but this is not the same as simply seeking attention.) On some level, they don't want to be noticed; they don't want anyone to recognize they have an ED. But on the other hand, they really want someone to notice, to help. So, they are torn.
I recently had a client come in and flat out admit this was the reason for her behaviors. I was impressed with her level of insight as it made it very clear what we needed to work on in that moment. However, for most, I think they are not even necessarily aware that they are using their body to communicate. I often ask patients what they are wanting someone to hear, and with whom they are trying to communicate. If you are family or friend, you could do a similar thing and ask your loved on what they want you to hear. You may learn a lot.
I also want to point out, I think this whole concept also applies very strongly to self-harm, particularly when wounds are visible to others. Again, this is VERY different from the easy answer of "attention-seeking." This is a deeper understanding of the person's internal battles.
So, that leaves us with the present reasons for the ED, what needs the ED meets. And even those are numerous, so today I am going to focus on just one: Eating disorders as a form of communication.
In comes the eating disorder. They can use their body to communicate how they feel. So, as their body size decreases or increases, they might be trying to say something that they cannot find the words for. (Note, this is different than that accusation of eating disorders being "attention-seeking." Yes, they are hoping someone will notice and help, but this is not the same as simply seeking attention.) On some level, they don't want to be noticed; they don't want anyone to recognize they have an ED. But on the other hand, they really want someone to notice, to help. So, they are torn.
I recently had a client come in and flat out admit this was the reason for her behaviors. I was impressed with her level of insight as it made it very clear what we needed to work on in that moment. However, for most, I think they are not even necessarily aware that they are using their body to communicate. I often ask patients what they are wanting someone to hear, and with whom they are trying to communicate. If you are family or friend, you could do a similar thing and ask your loved on what they want you to hear. You may learn a lot.
I also want to point out, I think this whole concept also applies very strongly to self-harm, particularly when wounds are visible to others. Again, this is VERY different from the easy answer of "attention-seeking." This is a deeper understanding of the person's internal battles.
Thursday, August 2, 2012
Ohhh, Group Therapy
In some groups, that power isn't very well managed, and the group results in everyone sinking into the abyss together. But, when a group is set on getting well and holds one another to that standard, then, THEN!, there's a ton of power. What an individual therapist or dietitian says that has minimal impact has so much more impact when it comes from a peer. Women who are used to being in the background, ignored, forgotten, suddenly are able to see that what they say matters, that it positively impacts others. Bonds are formed when the ED has made it so there are no connections. And, suddenly, all that initial anxiety was worth going through.
So, if you are in a group, and avoiding participation in some way, I encourage you to reconsider that. Group can be such a powerful and positive experience once you survive that initial anxiety (that, admittedly, can last quite a while). And if you are running and ED group and feeling at a loss for how to get the group process going, hang in there. Keep pushing the women to interact and overcome that anxiety. It will happen, and it will be worth it.
Give Us Some Feedback!
Hey! So, Blogger tells me people are reading this blog. And a couple of you have commented, but we'd love to hear from others! Is this blog helpful? Informative? Lowering your IQ as you read it? ;) Please, tell us what you think so we know whether to keep this up! Thanks!!
Tuesday, July 31, 2012
Nike: Just Do It!
Eating disorders are often so hard to understand for those who have not had one. Parents, friends and family often find themselves becoming so frustrated with their loved one who has an eating disorder because they can't understand why their loved one won't "just do it." They find themselves saying things like, "Come on, just eat!" or "If you wanted to get better, you'd do it." And, granted, some people with eating disorders don't want to get better at that moment, so maybe they really are not trying very hard, but at the same time, really, who chooses to have an eating disorder? And I think that is such a hard concept to work through when you are not the one struggling with this disorder. On the outside, it looks like a choice, it looks like something that could "easily" be changed by "just eating." So, what I try to help family and friends understand is that there is pretty much nothing rational about an eating disorder; thus, applying rational thought processes to the disorder just doesn't work very well. Oh, how tempting it is to rationalize with someone with an eating disorder, thinking, "if I can just get him/her to see the truth, she'll change!" But it is not that simple....
Eating disorders are (brace yourself for psychobabble) what is called ego-syntonic. What this means, basically, is that the ED helps the person in some way. Depression is usually ego-dystonic. People don't really want to have it, and when someone with depression comes into my office, they want me to help them get rid of it. EDs (and substance abuse, and self-harm), on the other hand, are "helping" the person. They help the person manage their emotions when they are so scared to face them straight on. They give the person an identity when he/she might feel invisible instead. They serve many, many purposes, which vary from person to person.
So, unfortunately, someone with an ED comes into my office partly wanting me to help them get rid of their disorder, and partly wanting to keep it so they feel safe. Many have what is called the "anorexic wish:" Please help me get over this disorder without gaining any weight. They don't want to have the disorder anymore, but they are terrified of weight gain, and honestly, they are terrified of life without the ED.
So, hopefully, now it makes more sense how the "just do it" approach doesn't work as well as we might hope. We can all relate to having emotions override rational thought, and how we act in those situations. So, for those with EDs, their fear overrides almost all rational thought on the subject. So, keep talking to your loved one rationally, but don't expect it to dramatically change their actions right then. It takes a lot to override fear. Early in treatment, "just do it" doesn't work.
 Though my patients would tell you I have been known, much later in treatment, to threaten that they must wear Nike clothes all the time to remind them that there does indeed come a time when, in recovery, you have to "just do it." But that is another post.
Though my patients would tell you I have been known, much later in treatment, to threaten that they must wear Nike clothes all the time to remind them that there does indeed come a time when, in recovery, you have to "just do it." But that is another post.
Eating disorders are (brace yourself for psychobabble) what is called ego-syntonic. What this means, basically, is that the ED helps the person in some way. Depression is usually ego-dystonic. People don't really want to have it, and when someone with depression comes into my office, they want me to help them get rid of it. EDs (and substance abuse, and self-harm), on the other hand, are "helping" the person. They help the person manage their emotions when they are so scared to face them straight on. They give the person an identity when he/she might feel invisible instead. They serve many, many purposes, which vary from person to person.
So, unfortunately, someone with an ED comes into my office partly wanting me to help them get rid of their disorder, and partly wanting to keep it so they feel safe. Many have what is called the "anorexic wish:" Please help me get over this disorder without gaining any weight. They don't want to have the disorder anymore, but they are terrified of weight gain, and honestly, they are terrified of life without the ED.
So, hopefully, now it makes more sense how the "just do it" approach doesn't work as well as we might hope. We can all relate to having emotions override rational thought, and how we act in those situations. So, for those with EDs, their fear overrides almost all rational thought on the subject. So, keep talking to your loved one rationally, but don't expect it to dramatically change their actions right then. It takes a lot to override fear. Early in treatment, "just do it" doesn't work.
Wednesday, July 25, 2012
The "perfect patient"
Many patients with eating disorders also have a significant problem with perfectionism. They want to be perfect, or the best, at most of what they do. And, for some, this includes being your "perfect patient." What does the perfect patient do? He/she tells you what you want to hear, acts as though everything is fine, and desperately wants your approval. So, whereas their morals may be against lying, they just might lie to you, just to make sure you are okay with them; their fear is to make you mad.

But, unfortunately, the "perfect patient," in my experience, rarely gets better. After all, what you want to hear is rarely what is really going on. What is really going on is incredible pain, torture, a horrible battle with an eating disorder. There's nothing pretty about this. And soon you start to see evidence of the "perfect patient." The concrete data (ie, weight, vitals, etc) doesn't match what the patient is reporting. The smile is strained and often barely held. You find there is not much depth to conversations. And, most of this is simply because your approval, acceptance, is what is so desired.
So, the "perfect patient" must learn that you will approve and accept them, even if everything isn't, well, so perfect. It become a challenge to balance the need for high expectations, which I believe are necessary for full recovery, with challenging the presentation as a "perfect patient." It is a challenge to balance the need for following a meal plan 100% with a patient's desire to tell you they did it when they didn't, just so you won't get mad. Really, I guess it all comes down to honesty and authenticity, and the trust that is built from keeping high expectations while also encouraging honesty. It is a balance, indeed. I also thinks this links to the patient's need to learn that, even if you do get upset with them (read: their eating disorder), you can work through it. They don't need to fake you out for you to be okay with them. You can simultaneously be upset at their eating disorder behaviors, and like them as a person. Said another way, you can dislike their ED, while liking them just fine. This is often a hard concept as the ED has become so ingrained as a part of the patient. But, separation is key.
I'm pretty sure nobody has ever said that recovery from, or treatment of, an eating disorder is very easy. It is hard, but oh-so-rewarding work.
Thursday, July 19, 2012
Secrets
There is a saying in addiction treatment that goes, "Secrets keep you sick." I first heard this phrase while working in a substance abuse RTC here in Salt Lake. There was a lot of focus in this program on secrets, letting secrets out, etc. This was such a powerful thing to be introduced to, and something I have carried with me since. I only wish I had been aware of this concept in the work I had done prior to working at this facility.

Over the years, it seems I have developed a somewhat uncanny ability to tell when someone is keeping a secret that is impeding their treatment. For some, I am sure this skill is quite irritating, but for many others, I can see the relief on their faces when I bring up the concept of holding onto secrets. Before going farther, I should probably better define what I mean by a secret.
 There's the obvious definition of a secret. Something you hold onto and don't tell anyone else. So, something you did, something that happened to you. And these can be powerful secrets. But, sometimes "emotional secrets" can be even more powerful. What I mean by this term is those emotions we feel, but don't tell anyone about. It's the emotions about events that we cannot escape and that we, for whatever reason, are too scared to tell anyone else about. Sometimes, we have told people the details of an event, so in that way, it is no longer a secret, but if we hold onto emotions about that event, suddenly it is still a secret. It's a hard concept to explain, but for those who you holding secrets, I am sure you know what I mean.
There's the obvious definition of a secret. Something you hold onto and don't tell anyone else. So, something you did, something that happened to you. And these can be powerful secrets. But, sometimes "emotional secrets" can be even more powerful. What I mean by this term is those emotions we feel, but don't tell anyone about. It's the emotions about events that we cannot escape and that we, for whatever reason, are too scared to tell anyone else about. Sometimes, we have told people the details of an event, so in that way, it is no longer a secret, but if we hold onto emotions about that event, suddenly it is still a secret. It's a hard concept to explain, but for those who you holding secrets, I am sure you know what I mean.
Secrets make people "act twitchy," as I often so clearly describe it. They generally avoid becoming emotionally connected, vulnerable, and when you ask a question, sometimes you can tell there's something not being said. They have emotional reactions to things that you can't quite understand. In many ways, it is hard to describe how to tell someone has a secret, and fortunately, most people don't need this skill. But, when clinicians have the ability to tell a secret is there, they can help the patient eventually feel safe enough to let it out.
 When it comes to eating disorders (or substance abuse, or self-harm), secrets will often lead the person to "need" the symptom to cope. This might be a strange concept to those of you who have not experienced one of these behaviors. How could someone "need" the symptom of a disorder? Well, when the emotions linked to a secret are so strong, and you are trying so hard not to let that secret out, the symptom serves as an excellent distraction, a way to avoid, and a way to keep others at arm's length.
When it comes to eating disorders (or substance abuse, or self-harm), secrets will often lead the person to "need" the symptom to cope. This might be a strange concept to those of you who have not experienced one of these behaviors. How could someone "need" the symptom of a disorder? Well, when the emotions linked to a secret are so strong, and you are trying so hard not to let that secret out, the symptom serves as an excellent distraction, a way to avoid, and a way to keep others at arm's length.
So, let's try an example. Let's say Suzie Q has an emotional secret. She feels extreme guilt about something she did a year ago, but that guilt makes it so she doesn't want to tell anyone because who knows what others will think of her. But, as she goes through her days, she thinks of this thing she did, and she feels badly. You can look at her sometimes, and see she seems to be lost in her own head, and she is thinking about that thing she did that she cannot tell you about. Sometimes that guilt becomes overwhelming and she almost cannot stand it, but then she engages in her ED. It doesn't matter the symptom; really, they all serve the same purpose. And as she engages in that symptom, she is distracted from that guilt, and maybe even feels better, because she is punishing herself. The guilt decreases for the moment. The problem is that the guilt always comes back, and it will until she is able to "work through" the guilt. So, the need for the ED symptom remains.
 Now, I can't say everyone with an ED has secrets. That would be unfair to draw such a broad stroke. But, if you have secrets that you have not told your treatment team about, maybe start by at least writing the secrets out; this way, you have at least admitted them to you. And, then, as you feel safe (not that it will ever feel TOTALLY safe to tell a secret), tell your team. Let them help you talk through it. And, fortunately, in my experience, once this happens, you will feel better. If it is your loved one that has secrets, I wouldn't try to force the secrets out....that is too scary and will be met with resistance. But, let your loved one know you are there to listen and to support whenever he/she is ready to talk.
Now, I can't say everyone with an ED has secrets. That would be unfair to draw such a broad stroke. But, if you have secrets that you have not told your treatment team about, maybe start by at least writing the secrets out; this way, you have at least admitted them to you. And, then, as you feel safe (not that it will ever feel TOTALLY safe to tell a secret), tell your team. Let them help you talk through it. And, fortunately, in my experience, once this happens, you will feel better. If it is your loved one that has secrets, I wouldn't try to force the secrets out....that is too scary and will be met with resistance. But, let your loved one know you are there to listen and to support whenever he/she is ready to talk.
Over the years, it seems I have developed a somewhat uncanny ability to tell when someone is keeping a secret that is impeding their treatment. For some, I am sure this skill is quite irritating, but for many others, I can see the relief on their faces when I bring up the concept of holding onto secrets. Before going farther, I should probably better define what I mean by a secret.
Secrets make people "act twitchy," as I often so clearly describe it. They generally avoid becoming emotionally connected, vulnerable, and when you ask a question, sometimes you can tell there's something not being said. They have emotional reactions to things that you can't quite understand. In many ways, it is hard to describe how to tell someone has a secret, and fortunately, most people don't need this skill. But, when clinicians have the ability to tell a secret is there, they can help the patient eventually feel safe enough to let it out.
So, let's try an example. Let's say Suzie Q has an emotional secret. She feels extreme guilt about something she did a year ago, but that guilt makes it so she doesn't want to tell anyone because who knows what others will think of her. But, as she goes through her days, she thinks of this thing she did, and she feels badly. You can look at her sometimes, and see she seems to be lost in her own head, and she is thinking about that thing she did that she cannot tell you about. Sometimes that guilt becomes overwhelming and she almost cannot stand it, but then she engages in her ED. It doesn't matter the symptom; really, they all serve the same purpose. And as she engages in that symptom, she is distracted from that guilt, and maybe even feels better, because she is punishing herself. The guilt decreases for the moment. The problem is that the guilt always comes back, and it will until she is able to "work through" the guilt. So, the need for the ED symptom remains.
Tuesday, July 17, 2012
On Anger....
I have heard a few times recently, "I don't really feel anger very much." Sometimes, of course, this is followed by statements about how and why anger is invalid, unnecessary, unacceptable. Now, ask the parents of a teenager with an eating disorder, and sometimes you will find there is plenty of anger being expressed. But the problem is that the vast majority, if not all, of the anger being expressed is about food, rather than about what really angers him/her.

However, I have noticed that, a lot of the time, those with eating disorders, especially anorexia, are seen as fragile, breakable, in need of being treated with kid gloves. I see it very differently. In my experience, behind a lot of eating disorders is a good amount of anger, but the individual does not feel anger is okay, so the anger leaks out in ED symptoms. In many ways, eating disorders are even somewhat aggressive disorders. Now, the actual person is not aggressive, but the disorder creates a level of aggressiveness.
Now, some would say that someone with an eating disorder is not in control of their behaviors and their actions, and sometimes that is true, but in my experience, it is not true as often as maybe providers assume. Certainly eating disorders dramatically impact brain functioning, but I'm not sure it is in such a way that the patient no longer has control over his/her actions.
So, back to the aggressiveness. Again, I want to be clear that I am NOT stating that those with eating disorders are intentionally aggressive. But, if you think of the behaviors, I think the anger behind them becomes more evident. Eating disorders require a lot of defiance; defiance of of bodily needs, others' expectations, treatment recommendations. They are not passive disorders, and thus, in my opinion, to treat them passively, rather than more directly confronting the disorder, may do a disservice to the person suffering with the disorder.
But, more importantly, in order for one to recover, he/she must deal with the underlying anger. It must be safe for him/her to express anger and that emotion must be accepted. I often encourage patients to get angry with me, which sounds kind of strange I am sure, but my goal is to make it clear it is okay to show anger, even anger at me. And I'm sure if you could ask the patients I work with, they will likely all confirm that I REALLY annoy them at some point, if not frequently. The key is, you must get past the anger at food, at treatment, at feeling controlled, and get to the "real" anger, the anger that comes from your experiences.

So, find a relationship where it's okay to be angry, and express away! For many patients I have worked with, as they have learned to express anger, they have found they have less need for their ED symptoms.
However, I have noticed that, a lot of the time, those with eating disorders, especially anorexia, are seen as fragile, breakable, in need of being treated with kid gloves. I see it very differently. In my experience, behind a lot of eating disorders is a good amount of anger, but the individual does not feel anger is okay, so the anger leaks out in ED symptoms. In many ways, eating disorders are even somewhat aggressive disorders. Now, the actual person is not aggressive, but the disorder creates a level of aggressiveness.
Now, some would say that someone with an eating disorder is not in control of their behaviors and their actions, and sometimes that is true, but in my experience, it is not true as often as maybe providers assume. Certainly eating disorders dramatically impact brain functioning, but I'm not sure it is in such a way that the patient no longer has control over his/her actions.
So, back to the aggressiveness. Again, I want to be clear that I am NOT stating that those with eating disorders are intentionally aggressive. But, if you think of the behaviors, I think the anger behind them becomes more evident. Eating disorders require a lot of defiance; defiance of of bodily needs, others' expectations, treatment recommendations. They are not passive disorders, and thus, in my opinion, to treat them passively, rather than more directly confronting the disorder, may do a disservice to the person suffering with the disorder.
But, more importantly, in order for one to recover, he/she must deal with the underlying anger. It must be safe for him/her to express anger and that emotion must be accepted. I often encourage patients to get angry with me, which sounds kind of strange I am sure, but my goal is to make it clear it is okay to show anger, even anger at me. And I'm sure if you could ask the patients I work with, they will likely all confirm that I REALLY annoy them at some point, if not frequently. The key is, you must get past the anger at food, at treatment, at feeling controlled, and get to the "real" anger, the anger that comes from your experiences.
So, find a relationship where it's okay to be angry, and express away! For many patients I have worked with, as they have learned to express anger, they have found they have less need for their ED symptoms.
Friday, July 6, 2012
One week vacation!
Just a note that Within Four Walls will be going on a one-week vacation, starting today. We hope to see you all back here in a week. Please feel free to leave any comments asking for topics to be addressed upon our return!
Thursday, July 5, 2012
The "War on Childhood Obesity"
I was asked to post on this topic, and first I wanted to research a bit more on the government's stance. First, on a government website, I found the announcement that a research task force has been developed, which seems quite reasonable. Then, however, I found an article (http://abcnews.go.com/GMA/Health/michelle-obama-childhood-obesity-initiative/story?id=9781473&page=2#.T_ZKbI64LzI) on Michelle Obama's push for the Childhood Obesity Task Force. And, a couple quotes caught my eye:
"I have set a goal to solve the problem of childhood obesity within a generation so that children born today will reach adulthood at a healthy weight," the text of the president's memorandum reads.
Perhaps this is a bit blunt, but this seems like such an ignorant statement. I am pretty sure the president is saying that the "healthy weight" is an average or below average weight. Of course, in reality, what do those terms even mean? But, anyway, I am pretty sure the president is not recognizing that weights are normally distributed, which is represented below.
If we assume weights are normally distributed, it means that some people are naturally very thin, and some people are naturally obese. This is where people's brains start scrambling. But, we all know someone who is naturally very thin. So, if you can accept that some people are naturally very thin, then you kind of have to accept some people are naturally obese.
So, back to the president's statement.... I'm pretty sure he is not accepting that some people's "healthy weight" actually falls within the obesity range. There is so much more that can be said about this, but to do so would make this particular post far too long, so let me know if you'd like to hear more. Next:
"To help parents, the first lady said she's working with the Food and Drug Administration and major food manufacturers and retailers to make it easier for parents to identify healthier foods by placing nutrition labeling on the front of the package."
Oh my! Who knew the problem was the location of the nutrition facts. Really? Enough said.
Now, this is just one article, so I realize it's not fair to base all my thoughts on this. So, more globally, I am concerned about any messages that identify good foods and bad foods, or healthy foods and unhealthy foods. This type of mindset violates the tenets of Intuitive Eating, which again is a whole 'nother post. But, to identify foods as "bad" or "unhealthy" just creates shame around eating those foods. And, even worse, sending the message that being "above average" in weight is "wrong" is horrifying, potentially creating long-lasting shame and self-hate.
I think there is much more benefit to teaching the benefits of carbs, proteins, fats, fruits and vegetables, than demonizing any specific types of food, and teaching how to read food labels, which, last I heard, are not even terribly accurate anyway. I don't have the citation, but last I heard, the FDA allows up to 20% error in a food label, which means if something says it has 100 calories, it could have anywhere from 80 to 120. How's this for a nutrition label, though?? (I suppose it should be placed on the front of the baby?)
In short, I think it is going to be very hard to skillfully teach about food in a school setting. The teacher will be biased by what he/she believes about food and pass on these biases. Now, if we could get a dietitian who teaches Intuitive Eating to go into every school and teach those concepts, that'd be awesome, but not practical. So, in the end, I cannot say what should happen. I just feel confident that demonizing food and being "above average weight" is NOT the way to go. And, as the last post addressed, making exercise about weight change ruins the fun of it, which, sadly, may decrease a kid's willingness to do it. So, I'm not sure the Obamas have hit the mark very well at all. I will hold out hope that the Task Force will receive information from researchers who truly understand the genetic, biological and psychological factors that impact obesity.
***Normal Distribution: Okay, statistics is a bit hard to blog on, but here's the basics. Imagine all the weights for all the women in the US who are 5'5" tall are on the graph above. All those dots would be within the blue line above....meaning between the blue line and the graph line along the bottom. So, the vast majority of dots would be near the middle, and that is why the curve is higher there; the height of the curve represents the number of dots. The middle would be the average weight for women 5'5" tall. But, out at the very ends, where the blue line is very close to the graph line, there would still be weights graphed there.
Tuesday, July 3, 2012
Exercise is healthy, right?
Oh, if I could count the number of times I say the phrase,
"Yes, exercise is good for you. Until it's an eating disorder symptom, and then it's bad for you."
Or,
"Yes, exercise is a good way to reduce anxiety, until it's an eating disorder symptom, and then it only serves to increase anxiety."
Exercise is the "socially acceptable way of purging." Really, using exercise to "get rid of food" is no different than any other form of purging. But, wow, we sure do give people a lot of attention for exercise, seemingly irregardless of situations where it is clear someone's exercise is not healthy, or they are not healthy. Of course, often exercise is a really good thing. But not always. And it shouldn't ever be about appearance.

Although our society is incredibly confused on this point, the intent of exercise is not to control weight or change appearance! If you really look at it physiologically, it's pretty simple. Exercise does NOT make you lose weight. Physiologically, exercise.....makes you hungrier! So, yes, you can lose weight by exercising. But, you also will have to not eat enough to support the exercise, for this to happen. If you follow hunger and fullness cues, exercise will just make you eat more.
So, it frustrates me that our society ruins exercise by making it all about weight loss. There are so many other purposes for exercise. Why do you exercise? (Please, no "to lose weight"s or "to change my appearance"s.)

And, please, rather than complimenting someone who exercises on their appearance, find something else to compliment. Let's try to override society's skewed view of exercise!

"Yes, exercise is good for you. Until it's an eating disorder symptom, and then it's bad for you."
Or,
"Yes, exercise is a good way to reduce anxiety, until it's an eating disorder symptom, and then it only serves to increase anxiety."
Exercise is the "socially acceptable way of purging." Really, using exercise to "get rid of food" is no different than any other form of purging. But, wow, we sure do give people a lot of attention for exercise, seemingly irregardless of situations where it is clear someone's exercise is not healthy, or they are not healthy. Of course, often exercise is a really good thing. But not always. And it shouldn't ever be about appearance.
Although our society is incredibly confused on this point, the intent of exercise is not to control weight or change appearance! If you really look at it physiologically, it's pretty simple. Exercise does NOT make you lose weight. Physiologically, exercise.....makes you hungrier! So, yes, you can lose weight by exercising. But, you also will have to not eat enough to support the exercise, for this to happen. If you follow hunger and fullness cues, exercise will just make you eat more.
So, it frustrates me that our society ruins exercise by making it all about weight loss. There are so many other purposes for exercise. Why do you exercise? (Please, no "to lose weight"s or "to change my appearance"s.)
And, please, rather than complimenting someone who exercises on their appearance, find something else to compliment. Let's try to override society's skewed view of exercise!
Monday, July 2, 2012
Relationships replace eating disorders
Treating eating disorders is difficult work, for both patient and provider. In reality, eating disorder treatment is a relatively new field, and the body of knowledge is growing exponentially each year. As a result, at times, we will seek advice from experts across the nation regarding how to approach a certain clinical situation. A few months ago, in response to one of these requests for suggestions, a number of conflicting ideas came in regarding how to broach a client's limited progress and difficulty adhering to treatment recommendations. And as all these ideas flew back and forth, there was one comment, quite simple really, that made it all make sense to me.
Now, I have no hope of getting the quote correctly, and unfortunately don't even remember who said it, but the bottom line was this....
As long as our clients believe in us as providers, whatever approach we take, within reason, is likely to "work."
And this confirms my belief about therapy, which is that, primarily, what we have to offer is a relationship. And then that relationship has power. And that power can join with the patient to create recovery from an eating disorder. I have seen patients with severe eating disorders symptoms choose to stop engaging in their eating disorder largely because a relationship finally matters enough to overpower the eating disorder. Sometimes, that relationship is with us as providers. Other times, it is with a child, a spouse, a family member.
I firmly believe relationships help replace eating disorders. Unfortunately, relationships are also what so often frighten those with eating disorders. Or probably all of us, really. So, what seems simple, is anything but.
And this confirms my belief about therapy, which is that, primarily, what we have to offer is a relationship. And then that relationship has power. And that power can join with the patient to create recovery from an eating disorder. I have seen patients with severe eating disorders symptoms choose to stop engaging in their eating disorder largely because a relationship finally matters enough to overpower the eating disorder. Sometimes, that relationship is with us as providers. Other times, it is with a child, a spouse, a family member.
I firmly believe relationships help replace eating disorders. Unfortunately, relationships are also what so often frighten those with eating disorders. Or probably all of us, really. So, what seems simple, is anything but.
But, overall, the idea that relationships can replace eating disorders this is good news, because we can all offer relationships, whether we are trained in doing so, or are a friend or family member.

And I thank all of my clients for offering me a relationship with them. There is no greater honor.
And I thank all of my clients for offering me a relationship with them. There is no greater honor.
Subscribe to:
Posts (Atom)