So, of course, the question is: How do you define recovery for yourself?
Wednesday, August 29, 2012
How do you define recovery?
So, of course, the question is: How do you define recovery for yourself?
Monday, August 27, 2012
Dieting causes obesity?
There are things that, in any field, because you are in it, you know it well. And then you think everyone else knows what you know, so of course they will follow it. But, then, in my case, my partner reminds me not everyone thinks the way we do about all this food, weight and exercise stuff. Which is kind of disappointing, you know.
 So, what we in this field know well is DIETING DOESN'T WORK! Oh, don't you worry, it has been researched to death. And that research resoundingly supports the understanding that 95-98% of diets will fail. Will you lose weight initially? Sure, some will, and they might even keep the weight off for a bit. But what the dieting industry leaves out of their marketing material is that 95-98% of people will regain the weight, and a good number of those will actually add 10% to their previous weight. Which, as you can imagine, reinforces starting another diet where they again regain the weight plus 10%. Surely you can see where this is going, right? People diet and actually gain weight! I was first introduced to this concept in my training in about 2002, and it shocked me. I thought, "You mean, in reality, dieting is a major cause of obesity?" Now, am I going to take the time to back up that claim here with research? No, I'm not. (I'm kinda lazy.) I throw it out as more of a discussion piece. But it certainly interesting how weights in the US have increased IN SPITE OF the proliferation of diets. Hmmmmm.
So, what we in this field know well is DIETING DOESN'T WORK! Oh, don't you worry, it has been researched to death. And that research resoundingly supports the understanding that 95-98% of diets will fail. Will you lose weight initially? Sure, some will, and they might even keep the weight off for a bit. But what the dieting industry leaves out of their marketing material is that 95-98% of people will regain the weight, and a good number of those will actually add 10% to their previous weight. Which, as you can imagine, reinforces starting another diet where they again regain the weight plus 10%. Surely you can see where this is going, right? People diet and actually gain weight! I was first introduced to this concept in my training in about 2002, and it shocked me. I thought, "You mean, in reality, dieting is a major cause of obesity?" Now, am I going to take the time to back up that claim here with research? No, I'm not. (I'm kinda lazy.) I throw it out as more of a discussion piece. But it certainly interesting how weights in the US have increased IN SPITE OF the proliferation of diets. Hmmmmm.
 What got me on this kick today was yet another high school acquaintance posting on Facebook how they are going to do something to lose weight. And, really, I don't know if it is the next fad diet, or perhaps worse, weight loss surgery. But each time this happens, I really want to contact these people who I have not spoken to in, uhhh, 19 years, and provide all the information we in this field know that goes counter to the diet industry. I mean, the diet industry has billions of dollars. The eating disorder field? Ahhh, not much. So, we will never be able to counteract the number of messages put out there by the dieting industry. And, that is frustrating.
What got me on this kick today was yet another high school acquaintance posting on Facebook how they are going to do something to lose weight. And, really, I don't know if it is the next fad diet, or perhaps worse, weight loss surgery. But each time this happens, I really want to contact these people who I have not spoken to in, uhhh, 19 years, and provide all the information we in this field know that goes counter to the diet industry. I mean, the diet industry has billions of dollars. The eating disorder field? Ahhh, not much. So, we will never be able to counteract the number of messages put out there by the dieting industry. And, that is frustrating.
But, if I did think it was advisable to contact each of the high school classmates, I would encourage them to work with a therapist to see if any ED behaviors underlie their weight problems. And to see a dietitian who can help them with Intuitive Eating, rather than just another diet. And tackling weight loss surgery is for another day, but these two recommendations (as long as the person sees actual eating disorder treatment experts) would address most concerns about weight loss surgery as well.
 But, alas, most people don't want to hear diets don't work. Until they have done enough of them that they cannot stand it for one more moment, and then many will open their minds to Intuitive Eating. And the dieting cycle and finally end.
But, alas, most people don't want to hear diets don't work. Until they have done enough of them that they cannot stand it for one more moment, and then many will open their minds to Intuitive Eating. And the dieting cycle and finally end.
But, if I did think it was advisable to contact each of the high school classmates, I would encourage them to work with a therapist to see if any ED behaviors underlie their weight problems. And to see a dietitian who can help them with Intuitive Eating, rather than just another diet. And tackling weight loss surgery is for another day, but these two recommendations (as long as the person sees actual eating disorder treatment experts) would address most concerns about weight loss surgery as well.
Thursday, August 23, 2012
High expectations
Because we know the impact of the eating disorder symptoms on the body, mood, functioning, social interaction, etc., we set terminating the symptoms as our initial primary goal. As a therapist, I am aware that trying to do therapy with someone in the midst of ED behaviors is of very limited benefit. One way to think about it is this: If you have an ED, how well do you remember your first, or probably even first few, therapy appointments. In the moment, you felt really with it and like you were fully functioning, and you likely even seemed to your therapist like you were totally with them, but reality is that very few patients remember those initial sessions. So, therapists can walk out thinking they just did excellent therapy but sadly, their therapeutic interaction had little effect because the physiological impact of EDs is so profound.
Dietary sessions are of course focused on ending ED symptoms, but in our model, so is therapy. The best way I can summarize it for patients, and now for you, is:
"Trying to do therapy with someone engaging in eating disorder symptoms is about as
effective as trying to do therapy with an alcoholic in a bar."
Imagine, I ask the inebriated alcoholic how he feels. Riiiiiight. How can therapy be done in that situation; the substance is masking the person's emotions. Same for an eating disorder.
And, I'll confess, I enjoy this second of stage much better than the first stage too.
Wednesday, August 22, 2012
Removing permission to purge
A couple years ago, admittedly a little further along in treating eating disorders than probably ideal, I noticed something. I noticed that when patients with bulimia talk about their symptoms, they would view bingeing and purging as essentially one symptom. And, so, for too long, I too responded as if they were one. When they are one symptom, though, bulimia is incredibly hard to treat. It seemed it was too much to give up both bingeing and purging at one time, and progress seemed to happen slowly.
Then, one day, it occurred to me that they were two separate symptoms, and should be treated as such. And, in that session, I finally realized that purging "allowed" bingeing to happen. As long as the person had "an out" (please do not read this as saying people WANT to purge, that is not my point) with purging, they were "more able" to binge. So, I started with that one patient and talked to her about the possibility of "removing the permission to purge." We talked about how, if she were to no longer allow herself to purge, would she binge? And she admitted that, without purging as an option, she would not be as likely to binge.
So, we moved forward with this concept of "removing the permission to purge," and sure enough, she first stopped purging, and shortly thereafter, stopped bingeing. Now, as this happened, we of course had to deal with all the underlying emotions and thoughts that came up as those ED symptoms were terminated; I make it sound simple here, but it is anything but, I know. But there seemed to be a lot of power in the concept of "removing the permission to purge."
Since, I have introduced this concept to each patient I work with who engages in bingeing and purging. And, as with many things I propose, patients first look at me like I have grown a second head and most certainly lost my mind, but as we talk about the rationale, they eventually become willing to give it a try. It would be ideal if refusing purging meant one never binged again, but that simply isn't the case most of the time. Most patients have been in the position of having to "sit with" a binge, but time and again, that sitting through a binge without purging has created enough of a negative experience that the patient's bingeing decreases dramatically, if it doesn't stop completely. Patients talk about feeling more in control, more confident, and feeling less pull from the eating disorder symptoms.
Of course, once the symptoms stop, the real therapy begins, so they are far from cured. But as I will discuss in another post, the symptoms must stop first for the deeper work to begin.
So, consider it....what impact would it have on your eating disorder if you "removed the permission to purge?"
Then, one day, it occurred to me that they were two separate symptoms, and should be treated as such. And, in that session, I finally realized that purging "allowed" bingeing to happen. As long as the person had "an out" (please do not read this as saying people WANT to purge, that is not my point) with purging, they were "more able" to binge. So, I started with that one patient and talked to her about the possibility of "removing the permission to purge." We talked about how, if she were to no longer allow herself to purge, would she binge? And she admitted that, without purging as an option, she would not be as likely to binge.
So, we moved forward with this concept of "removing the permission to purge," and sure enough, she first stopped purging, and shortly thereafter, stopped bingeing. Now, as this happened, we of course had to deal with all the underlying emotions and thoughts that came up as those ED symptoms were terminated; I make it sound simple here, but it is anything but, I know. But there seemed to be a lot of power in the concept of "removing the permission to purge."
Since, I have introduced this concept to each patient I work with who engages in bingeing and purging. And, as with many things I propose, patients first look at me like I have grown a second head and most certainly lost my mind, but as we talk about the rationale, they eventually become willing to give it a try. It would be ideal if refusing purging meant one never binged again, but that simply isn't the case most of the time. Most patients have been in the position of having to "sit with" a binge, but time and again, that sitting through a binge without purging has created enough of a negative experience that the patient's bingeing decreases dramatically, if it doesn't stop completely. Patients talk about feeling more in control, more confident, and feeling less pull from the eating disorder symptoms.
Of course, once the symptoms stop, the real therapy begins, so they are far from cured. But as I will discuss in another post, the symptoms must stop first for the deeper work to begin.
So, consider it....what impact would it have on your eating disorder if you "removed the permission to purge?"
Tuesday, August 21, 2012
Stumped
I'm thinking more seriously about writing a book on ED treatment, which of course would be an incredibly difficult endeavor, and then there's the reality that there are so many ED books out there. But I really love helping others learn more about treating EDs. Not that I/we have all the answers, but I think we do have a lot to share. I guess for now, I will just have to research the publishing world to see if I have the guts to enter it.
In short, I wonder if the type of book I would want to write is really wanted, or would be very respected. It is very hard to know, and I'd really like to avoid that whole rejection thing! Yep, I prefer to avoid rejection also; don't we all?
I dunno, are there any topics you'd like to hear about? I'm open to about anything....as long as I don't have to do research, apparently!
Monday, August 20, 2012
EDs as a form of communication
Of course, eating disorder 101 is "it's not about the food." Oh, it seems like it is about the food, and one really good way to irritate a patient in the midst of an eating disorder is often to tell them that, in reality, their eating disorder is not about the food.
 I have gotten many a nasty look and deep sigh in response to that one! But I persist on my statement, much to the client's chagrin.
I have gotten many a nasty look and deep sigh in response to that one! But I persist on my statement, much to the client's chagrin.
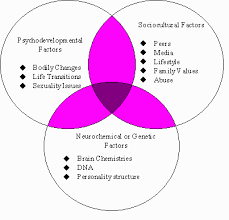 Eating disorder 101, part two, is that very few people will ever know "why" they have an eating disorder. In my 10 years of doing this, and hundreds of patients, I can now say I "know why" a whopping two patients have their eating disorder. For the other hundreds, well, there are just too many reasons. And, reasonably so, most people, and their families want to know why. But, reality is, it is a combination of a number of factors, some genetic and some environmental, and we can almost never identify the why.
Eating disorder 101, part two, is that very few people will ever know "why" they have an eating disorder. In my 10 years of doing this, and hundreds of patients, I can now say I "know why" a whopping two patients have their eating disorder. For the other hundreds, well, there are just too many reasons. And, reasonably so, most people, and their families want to know why. But, reality is, it is a combination of a number of factors, some genetic and some environmental, and we can almost never identify the why.
So, that leaves us with the present reasons for the ED, what needs the ED meets. And even those are numerous, so today I am going to focus on just one: Eating disorders as a form of communication.
 Many individuals with eating disorders struggle to put words to their feelings. Add to that their social isolation and tendency to keep others at a distance, and very rarely will you find an ED patient with a strong social support network with whom they talk openly. They have often lost the ability to walk up to someone and say, "I'm really sad about....," or "I'm so mad that you....."
Many individuals with eating disorders struggle to put words to their feelings. Add to that their social isolation and tendency to keep others at a distance, and very rarely will you find an ED patient with a strong social support network with whom they talk openly. They have often lost the ability to walk up to someone and say, "I'm really sad about....," or "I'm so mad that you....."
In comes the eating disorder. They can use their body to communicate how they feel. So, as their body size decreases or increases, they might be trying to say something that they cannot find the words for. (Note, this is different than that accusation of eating disorders being "attention-seeking." Yes, they are hoping someone will notice and help, but this is not the same as simply seeking attention.) On some level, they don't want to be noticed; they don't want anyone to recognize they have an ED. But on the other hand, they really want someone to notice, to help. So, they are torn.
I recently had a client come in and flat out admit this was the reason for her behaviors. I was impressed with her level of insight as it made it very clear what we needed to work on in that moment. However, for most, I think they are not even necessarily aware that they are using their body to communicate. I often ask patients what they are wanting someone to hear, and with whom they are trying to communicate. If you are family or friend, you could do a similar thing and ask your loved on what they want you to hear. You may learn a lot.
I also want to point out, I think this whole concept also applies very strongly to self-harm, particularly when wounds are visible to others. Again, this is VERY different from the easy answer of "attention-seeking." This is a deeper understanding of the person's internal battles.
So, that leaves us with the present reasons for the ED, what needs the ED meets. And even those are numerous, so today I am going to focus on just one: Eating disorders as a form of communication.
In comes the eating disorder. They can use their body to communicate how they feel. So, as their body size decreases or increases, they might be trying to say something that they cannot find the words for. (Note, this is different than that accusation of eating disorders being "attention-seeking." Yes, they are hoping someone will notice and help, but this is not the same as simply seeking attention.) On some level, they don't want to be noticed; they don't want anyone to recognize they have an ED. But on the other hand, they really want someone to notice, to help. So, they are torn.
I recently had a client come in and flat out admit this was the reason for her behaviors. I was impressed with her level of insight as it made it very clear what we needed to work on in that moment. However, for most, I think they are not even necessarily aware that they are using their body to communicate. I often ask patients what they are wanting someone to hear, and with whom they are trying to communicate. If you are family or friend, you could do a similar thing and ask your loved on what they want you to hear. You may learn a lot.
I also want to point out, I think this whole concept also applies very strongly to self-harm, particularly when wounds are visible to others. Again, this is VERY different from the easy answer of "attention-seeking." This is a deeper understanding of the person's internal battles.
Thursday, August 2, 2012
Ohhh, Group Therapy
In some groups, that power isn't very well managed, and the group results in everyone sinking into the abyss together. But, when a group is set on getting well and holds one another to that standard, then, THEN!, there's a ton of power. What an individual therapist or dietitian says that has minimal impact has so much more impact when it comes from a peer. Women who are used to being in the background, ignored, forgotten, suddenly are able to see that what they say matters, that it positively impacts others. Bonds are formed when the ED has made it so there are no connections. And, suddenly, all that initial anxiety was worth going through.
So, if you are in a group, and avoiding participation in some way, I encourage you to reconsider that. Group can be such a powerful and positive experience once you survive that initial anxiety (that, admittedly, can last quite a while). And if you are running and ED group and feeling at a loss for how to get the group process going, hang in there. Keep pushing the women to interact and overcome that anxiety. It will happen, and it will be worth it.
Give Us Some Feedback!
Hey! So, Blogger tells me people are reading this blog. And a couple of you have commented, but we'd love to hear from others! Is this blog helpful? Informative? Lowering your IQ as you read it? ;) Please, tell us what you think so we know whether to keep this up! Thanks!!
Subscribe to:
Comments (Atom)